
Rebecca Dekker
PhD, RN
Evidence on: Doulas
Originally published on March 27, 2013, and updated on April 17, 2024 by Rebecca Dekker, PhD, RN, Sara Ailshire, MA, and Ihotu Ali, MPH. Please read our Disclaimer and Terms of Use. For a full length printer-friendly PDF, become a Professional Member to access the complete library.
What is a doula?
A doula is a special companion who supports you during pregnancy, labor, and birth (Morton & Clift 2014). Doulas are trained to provide continuous, one-on-one care, physical support, and emotional support during labor. They may also provide information and support to families before or during birth, and into the postpartum period. There are many different types of doulas, along with many different types of training, certifications, traditional practices, and perspectives on doula care.
In this Signature Article, we provide families with evidence they can use when deciding whether and how to work with a doula. Making the evidence on doula care accessible can also educate communities, show the value of doulas to hospitals or medical providers, and help people advocate for policies that embrace doulas. Evidence shows that doulas are valued members of the care team who help improve health outcomes for parents and babies.
Read the Podcast Transcript
Dr. Rebecca Dekker – 00:00:00:
Hi everyone, on today’s podcast, we’re going to talk about the Evidence on Doulas. Welcome to the Evidence Based Birth® Podcast. My name is Rebecca Dekker, and I’m a nurse with my PhD and the founder of Evidence Based Birth®. Join me each week as we work together to get evidence-based information into the hands of families and professionals around the world. As a reminder, this information is not medical advice. See ebbirth.com/disclaimer for more details.
Hi everyone, and welcome to today’s episode of the Evidence Based Birth® Podcast. My name is Dr. Rebecca Dekker, pronouns she/her, and I’ll be your co-host for today’s episode. Today, along with co-host Sara Ailshire, we are excited to bring some brand new evidence-based information to you all about the evidence on doulas. As a quick content note, we will talking about the impact of racism on birth outcomes, as well as homophobia and transphobia, birth trauma, and obstetric violence. Today with me, I have Sara Ailshire. Sara, pronouns she/her, is a doctoral candidate in anthropology and an Evidence Based Birth® research fellow in her second year here at EBB. Sara, we’re so excited to have you here.
Sara Ailshire – 00:01:17:
Thank you so much. I’m especially excited to be talking with you today about doulas because in addition to my work here at EBB, my own academic research has in part focused on the efforts of birth practitioners like doulas to improve people’s experiences in childbirth. I’ve had the privilege to learn a lot from doulas over the years, and I hope I’m doing their legacy of mentorship proud when I’m doing work here at EBB.
Dr. Rebecca Dekker – 00:01:44:
So Sara, you came on the team in 2023 and you’ve been very busy the past year. You worked with us on nitrous, PROM, pre PROM, preterm PROM, and skin-to-skin after Cesarean. You also did the year-in-review podcast with us. So now we’re moving on to talk about the Evidence on Doulas, which is a project that you helped with along with Ihotu Ali. And we had never published a podcast episode focusing on the Evidence on Doulas. So for all of you listening, this is the first one. We’ve had lots of doulas interviewed on the podcast. We’ve never talked, done an overview of the Evidence on Doulas. However, we have had a Signature Article on the Evidence on Doulas that was published in 2013, updated in 2017 and 2019. And so today’s episode is celebrating the 2024 update of our Signature Article on doulas, which is now available at the Evidence Based Birth® website. Just go to ebbirth.com/doulas and you can download a free one-page handout on this topic that is easily downloadable at the top of the page.
So this doula article update is a project we started working on in 2023. And it was co-authored by Sara, myself, and Ihotu Ali, who is a doctoral student with her MPH, who also contributed substantially to this article. So our goal with this article is to write it both for people who may be interested in hiring a doula and also for doulas themselves or people who might be interested in becoming a doula. It has a really broad scope. In this article on doulas, we cover what a doula is, what are the benefits of having a doula, how is having a doula present at birth different from having your spouse or partner’s companionship, why doulas are so effective, what are some of the newer research finding on doulas, what do the professional guidelines say from midwives and doctors about doulas, and of course, we always end by talking about what is the bottom line on the evidence on doulas. So Sara, I would love for you to kick us off and start off by explaining what a doula is.
Sara Ailshire – 00:03:51:
Sure. So a doula is a special companion who supports you in labor and birth. In general, doulas are trained to provide continuous one-on-one care. They provide physical support and emotional support during labor. Doulas can also provide informational support to new parents and expecting families. They can give some general guidance about, you know, information about childbirth, things that they could expect to see in the hospital, just kind of preparing people for what birth could look like. Doulas can also be a source of advocacy during and after birth. Finally, a lot of people will receive some follow-up care after they’ve had their baby from their doula. They’ll maybe meet with them one time and reflect on the experience and get some guidance. There’s lots of different types of doulas, though. And there’s lots of different types of trainings and certifications, traditional practices, and perspectives on doula care. An anthropologist by the name of Dr. Dana Raphael is the person who kind of coined the term doula to describe labor companions. She first did this in her dissertation all the way back in 1966. But she really popularized the term and kind of brought it into the mainstream through a book that she published in 1973 called the Tender Gift: Breastfeeding. However, birth companions have been present in all cultures and across all time periods. Modern doulas today may be carrying on this legacy of companionship and support, but they didn’t invent it and it didn’t start, you know, in America in the 1960s. The use of the term doula is newer, but this concept of birth work is deeply rooted in human history.
Dr. Rebecca Dekker – 00:05:33:
Yeah, and before we go any further, I want to share a quick note about the term doula. So in this article, in this podcast, we use that term because it’s the most widely used word to describe birth companionship and support. However, there are other words that may be used for this role. You may see the term birth worker, birth sister, perinatal community health worker, among others. And we have seen that some birth workers reject the term doula because of its history of meaning slave or servant in Greek culture. Others feel that the term doula does not address the whole of their work or that other words might make more sense to their communities. So while we’re using the term doula and while we’re focusing on the research on doulas, please note that birth companionship does not begin or end with this terminology. I also want to point out that in many countries, the role of a traditional birth attendant, a midwife, and a doula are considered distinct roles from one another. However, the separation of these roles is a relatively recent development in history.
So for those of you who are not aware, a traditional birth attendant or traditional midwife may refer to birth companions who attend births and catch babies, but they do not have legal status within their state or country as a licensed midwife. And traditional birth attendants are continuing the ancient tradition of supporting birthing people, either from family members who have given birth previously or a member of the community who has a specialized expertise in birth work. And in some cultures, there’s other special words for these birth practitioners, such as gyn, grand midwife, comadrona, and more. So we also have midwives who practice in medical settings and different types of midwives with different scopes of practice, training, or licensure. And so although today people consider these traditional birth attendants, midwives, and doulas to be distinct, we want to point out these lines were blurred in the past and still are in some places.
And another note before we dive deeper into the evidence on doulas is that, here at Evidence Based Birth®, we recognize that the late 1900s movement to train and certify doulas was initially led by white doula trainers who worked to “professionalize” these birthing practices that had been preserved across cultures by Black, Brown, and Indigenous women. And some of these organizations claimed superiority in their field. They appropriated from and failed to credit the ancestral skills and cultural knowledge preserved by these Indigenous Black and Brown communities aroud the world. and the problems in Doula work have been similar to the problems of the North American Women’s Health Movement, which is a collective name for feminist activist efforts in reproduction. But today there are many programs all around the world that are training and certifying doulas. A growing number of doula organizations in the United States are led by people of color. And some traditionally white-led doula organizations have taken steps to address racism and promote diversity within their organizations, but the work is ongoing. It’s a work in progress.So Sara, take us back, you know, as we start going into the research, I think it might be helpful to know some of the terms about the different types of doulas. So can you walk us through the different types that are available?
Sara Ailshire – 00:09:00:
Yeah, absolutely. And these are just sort of like a sampling of common types of doulas you might see, like in addition to somebody who describes themselves as a doula. They may have additional training or additional experience in these elements of doula care. Because it’s a really, you know, it’s a broad, it’s a big umbrella. It’s a big tent. So community-based doulas are doulas who are, you know, who have doula skills who come from the same communities as their clients. They may oftentimes develop really close relationships with their clients. They may know them already or have a social connection to them. And in addition to providing them with birth support, they may also assist them in getting signed up for, you know, beneficial programs. They might help them address like other issues that they’re facing in their lives or in their relationships. They can really offer wraparound care for the people that they’re supporting in birth and pregnancy. And in some cases, community-based doulas may have really long lasting relationships with their clients. Like it doesn’t just sort of start and stop after their client has given birth. Postpartum doulas are doulas who are trained to provide support to birthing people and their families in the weeks following birth.
So they provide families with support and information about infant care and feeding, soothing. If it’s their first baby, they might be, you know, there to kind of help people ease into that role. And that can include not just the birthing person, but their partner. If it’s a family that already has children, they may also provide support to, you know, siblings as they like adapt to this new family member. Some postpartum doulas will also provide care to new families by assisting with light household tasks. It may help provide nutritious foods. It gives you a variety of things for people in the weeks following birth. Full-spectrum doulas are doulas who provide support before, during, and after pregnancy. This can include support during and after abortion care. End-of-life doulas, who are sometimes called deaf doulas colloquially, are people who are trained in some of the same ethos of being a doula, of being a present, knowledgeable, supportive companion. But instead of accompanying people around the beginning stages of life, they’re accompanying them as they leave this life and enter what comes next. And they provide support not only to a dying person, but again, to their community, to their family. Last-end bereavement doulas are doulas who specialize in providing support to childbearing families who have experienced a miscarriage, a fatal fetal diagnosis, a stillbirth, or an infant loss. And in episode 195, I think, Rebecca, you spoke with a full-spectrum doula who also offered loss and bereavement doula care services, right?
Dr. Rebecca Dekker – 00:11:51:
Yeah. And I also think one of the doulas you mentioned, I want to clarify the community-based doula. Sometimes people say, well, I practice in my community, so I’m a community-based doula. But that is a special term reserved typically for doulas who are from the same marginalized group as their clients. Not anybody can call themselves a community-based doula, if that makes sense. I think the people that typically we have hired in the past as doulas, you might think of as more of, some people call them a traditional, but I would say a better word might be like a typical doula that’s gone through a typical training and provides several prenatal visits, the birth support, and one postpartum visit. That would be like more typical. And the community-based doula is a much more in-depth, broad-ranging support.
Sara Ailshire – 00:12:39:
Yeah, absolutely. And a lot of, I think, community-based doulas too will work with organizations or work with other community-based doulas to provide care like within their community. Is that right?
Dr. Rebecca Dekker – 00:12:49:
Right. Yeah, exactly. And somebody could practice in both methods as well. They might have a more typical standard practice and then also do community-based work as well. So we often see some people will be doing this typical birth doula. They may be a postpartum doula. So people can have more than one role as well.
Sara Ailshire – 00:13:09:
Yeah, absolutely. And that’s the thing that is so interesting. Doulas can do a lot of different things and develop these trainings over time. But I think it might also be helpful to talk about what doulas are not. What I think sometimes people can be a little bit confused about what is the role of a doula and how is a doula distinct from other types of birth professionals, other types of medical practitioners, things like that. Well, for starters, doulas are not nurses and they’re not medical professionals. And having a doula present with you when you’re giving birth is very distinct from having a chosen companion like your partner, relative or friend providing you labor support. Doulas do not perform clinical tasks like cervical exams or fetal heart monitoring. They’re not supposed to give medical advice or give you a diagnosis. They might say, hey, that sounds serious. You should talk to your midwife. You should talk to your OB. But they’re not going to be able to tell you like, oh, you definitely have this, this or this. Doulas do not make decisions for you. Those can help you evaluate your options can help you through the decision-making process.
But ultimately, the role of a doula is support, not deciding for somebody. They’re not supposed to pressure you into adhering to their preferences or their, you know, their choices. They do not take over for the partner. A lot of partners find that doulas are supporting them almost as much as they’re supporting the birthing person. They can really benefit from that relationship. But doulas don’t take over. They don’t catch the baby. And in general, doulas don’t change shifts. So like most of them, when you have a doula, a doula will be with you during labor and birth. In some cases, doulas may call-in backup if birth goes on or labor goes on for a long time. Or if you’re giving birth in a hospital and there’s volunteer doulas or doulas who are working through the hospital, that might be a case where you see a doula shift change. But in general, a doula is kind of assigned to you and sticks with you throughout the process. We talked about this a little bit already, but in addition to all different types of doulas, there’s also a lot of different types of doula trainings that people can pursue. And there’s different philosophies about how to become a doula in the first place. So something that we wanted to do in the article was we wanted to share some information that clarifies the different pathways that people take to becoming a doula. Not only to benefit people who are interested in working with doulas, but ideally to support people who are interested in taking on this work who might want to become a doula themselves.
We also thought this information could be really helpful for those who are interested in hiring a doula and are trying to explain, maybe to their partner or to their family members, who this person is and what they do and how are they qualified to support you in this life experience? Some other things that we added to the article was, we were able to expand a little bit on the types of support the doulas provide. So we talked a little bit about The Four Pillars of Labor Support. We introduced little bit more information about the types of physical support, emotional support, informational support, and advocacy support that doulas can offer. And we did that because we really wanted to emphasize, again, a big variety of doulas, big variety of doula trainings, a lot of different ways of thinking about how to approach birth, how to be a doula. We want to support doulas and clients in finding the right match, finding somebody whose expectations are going to align in the best possible way with the doula that they’re going to work with. Not all doulas approach things the same way. And it’s really important that both people feel respected, heard, and feel that it’s a good fit for one another. So to help facilitate this, we also developed an interview guide that we include at the end of the Signature Article that prospective clients could use when they’re interviewing different doulas and that maybe doulas could use with their clients to kind of help structure these conversations around, you know, what are your expectations? What are your needs? Like, and how does that align with the professional services that doulas offer? Just to ensure that everybody leaves the birth experience feeling satisfied and respected.
Dr. Rebecca Dekker – 00:17:38:
Yeah. I want to congratulate you on helping create that interview guide. That was like, I think a really helpful addition to the end of the article. And I also wanted to give a couple of examples of it, if it’s okay, of the different types of support. So with physical support, we give a bunch of examples, but this could include creating a calm environment, such as dimming lights, arranging curtains, applying warmth, or cold packs, holding your hand, keeping eye contact with you, if that is helpful, guiding you with position, swaying movement, using a birth ball or peanut ball. And in low resource settings, doulas may alert the staff. If you have unusual symptoms that they’re not addressing, they may offer interpretation support. If there is a low resource area and you’re not getting the interpretation you need emotional support with like helping you feel more in control, more confident, showing a caring attitude, mirroring back to the emotions and feelings you’re having, showing just complete acceptance of your wishes, debriefing after the birth and really listening to empathy.
A lot of doulas we know love Evidence Based Birth® because they use our materials to help educate you. So they are working on helping find evidence-based information about different options. They’re pretty good at being able to explain common medical procedures and help you with communication. And of course, the more controversial aspect of doula support is advocacy support, which we define as supporting the birthing person in their right to make decisions about their own body and baby. And this is a bit controversial. We go into the background of this subject and we give some examples of subtle advocacy that I think most doulas would feel comfortable using, such as asking you what you want in front of your care team, encouraging you to ask questions, verbally supporting your decisions, helping facilitate communication. But we also give examples of more direct advocacy techniques, such as like amplifying your voice if you’re being dismissed, ignored, or not heard. For example, a doula could say, excuse me, like they’re trying to tell you something. I wasn’t sure if you heard them or not. They could say that to the provider. They could fill communication gaps. They could ask to speak with a nurse in the hallway, let them know that something is triggering for you, if you’re a survivor. Informing the nurse or physician, you really need to get an interpreter, you know, reminding the care team of your wishes and alerting the care team to concerning signs or symptoms, such as excessive blood loss or signs of preeclampsia. So I hope I didn’t go too far off track, but I think it was important to mention that you can go straight to the article and find just all these examples of ways doulas support families. And it’s so invaluable.
Sara Ailshire – 00:20:29:
No, absolutely. I think it’s really helpful to have those examples. Just so if you’ve never given birth before, never worked with a doula before, you can also kind of imagine, okay, like what would be useful for me? Like what should these would work? And also I think just gives everybody an appreciation for the incredible support and care that doulas offer to birthing people in all sorts of different dimensions. So Rebecca, I wanted to ask you if you wouldn’t mind sharing a little bit about what does the evidence show about the benefits of having a doula?
Dr. Rebecca Dekker – 00:20:59:
Yeah. So I want to share three studies with you all. So the first one is a Cochrane review by Boren et al. Published in 2017. This combined the results of 26 randomized controlled trials with more than 15,000 participants across 17 countries all over the world in both high-income and middle-income settings. And so people in these studies were randomly assigned like flipping a coin to either receive continuous one-on-one labor support or usual care. One of the things that I think is important to keep in mind is because these were randomized trials, you have equal numbers in both the doula group and the usual care group of people who desire an unmedicated birth or have certain preferences for their birth. So that controls for differences in the population. That’s why we do randomized control trials. I think some people get confused because they’re like, well, the Doula results are better because people wanted to work with a Doula. But that’s not the case. It’s like flipping a coin. You don’t get to control in these studies if you have a Doula or not. And in this review, it wasn’t just doulas. Continuous support can also be provided by other hospital staff, such as a midwife or a nurse or a companion from the family’s social network.
In 15 of these studies, the birthing person’s partner was not allowed to be present at the birth at all. And unfortunately, that is still something that happens in parts of the world, especially areas where you have no privacy, so they can’t let male companions into the labor ward. In the other 11 studies, the partner was allowed to be present in addition if they were assigned to somebody else for labor support. Overall, they found that those who received continuous labor support were more likely to have spontaneous vaginal births, less likely to need pain medication, less likely to have epidurals, less likely to have negative feelings about their birth, and less likely to have vacuum or forceps assistance or Cesareans. In addition, their labors were shorter by about 40 minutes on average, and their babies were less likely to have low Apgar scores at birth. An Apgar score is a measure of the baby’s immediate health at birth. There was also some evidence that doula support in labor lowered rates of postpartum depression afterwards, and they found no evidence that there were any risks to doula support. So it was a risk-free intervention that improved health outcomes. And they found that overall doulas are safe and beneficial.
Now, they also looked to see how, you know, if the type of support maybe different. So, does it matter who is there with you providing continuous labor support? Does a midwife, a doula, a partner, a friend, or relative offer more benefit? And they were able to look at this question for six topics. Use of any pain medication, use of pitocin during labor, a spontaneous vaginal birth, which means a vaginal birth that happens on its own without forceps or vacuum, Cesarean rates, admission to the special care nursery after birth, and negative birth experiences. So, the researchers found that for two of the health outcomes, the best results occurred when someone had continuous labor support from a trained doula. So this person was not a staff member at the hospital, and they were not part of the client’s social network. And the researchers found that overall, continuous support during birth led to a 25% decrease in the risk of Cesarean, and the largest effect was seen with a doula, a 39% decrease in the risk of Cesarean. A 8% increase in the likelihood of spontaneous vaginal birth, and the largest effect was seen with a doula. That was a 15% increase. A 10% decrease in the use of any medicines for pain relief, shorter labors by 41 minutes on average, a 38% decrease in the baby’s risk of a low five-minute Apgar score, and a 31% decrease in the risk of being dissatisfied with the birth experience. Basically, they’re finding that continuous labor support is important and beneficial, and we can make at least two of these outcomes even better if you have labor support from a trained doula.
In a later Cochrane review that was published in 2019, also by Boren et al., this was looking more qualitatively at women’s experiences during childbirth. So they found 51 studies, mainly from high-income countries, and they found that having a labor companion positively influenced the dynamic between birthing families and their healthcare providers. They found that the presence of a labor companion helped protect women from mistreatment in childbirth and improved health outcomes because the labor companions noticed and called attention to potential complications throughout labor and birth. They also found that most people in the studies wanted and benefited from the presence of a labor companion, whether it was a trained doula or a family member, partner, or friend.
And then the third study I’m going to talk about is a 2022 systematic review, where researchers combined nine studies with nearly 7,000 participants, and they were exploring the benefits of having a female relative act as a Lay Doula. So a Lay Doula would mean somebody who has not been formally trained as a doula, but they’re kind of acting in that role. And, you know, we’ve had people on the podcast come on and talk about, my mom acted like my doula, or my sister acted like my doula. So the results from this study showed that birthing people consistently reported positive birth experiences when their female relatives served as lay doulas. However, the lay doula’s impact on the Cesarean risk and the length of labor was inconsistent. Some studies showed that lay doulas had a positive impact on these things. Others found no difference. But overall, the review found that positive benefits of continuous labor support are most beneficial if you also have a formally trained doula with you who is not hired by the hospital. And that’s where you get the benefit of lowering the Cesarean rate. So, Sara, I talked a little bit about the lay doulas. Can you go into more depth and talk about how having a trained doula at your birth would be different from having your spouse or a partner’s companionship?
Sara Ailshire – 00:27:38:
Yeah, absolutely. So some people think that, you know, they hear about doulas and like, well, why would I need that? My partner is going to be there for me. My friend’s going to be there. I’m going to have the person who is closest to me present. And it’s true that having your chosen labor companion with you is essential and it’s really beneficial for you to have that person by your side. But that person is also going to need to do things. They’re going to need to eat and they might need to use the bathroom. And more than that, they might just need support in their own emotional journey. They might become overwhelmed, especially if they, you know, if they’ve ever seen a birth before or, you know, if you’re moving through labor. And you’re maybe vocalizing a lot and they’re distressed because they think you’re distressed. They just might not know what’s going on.
So having a person who has training and experience, who’s knowledgeable about childbirth can be really, really beneficial. Having somebody there who has knowledge about common medical procedures. What if you’re in a hospital setting, what is normal? What goes on there? And doulas are people who have this knowledge and who have this experience. And they will use that not only to support the birthing person, but to support and inform their labor companion, their partner. So that’s a really important distinction. Basically, a doula can provide the experience, provide the knowledge, provide, you know, the guidance through the emotional aspects of birth in order to kind of not only support the birthing person, but to support the birthing companion in supporting the birthing person. Doulas can educate partners, not only about birth, but you can also educate them about how to advocate for their spouse or for their friend. And they can work together with partners to kind of make up a labor support team.
Research has shown, so I’m going to talk a little bit here about fathers in particular, but research has shown that the most positive birth experiences for fathers were ones where they had continuous support from either a doula or a midwife. In these research studies, these fathers reported that they really benefited from having a person who had the time to explain things to them, who could answer their questions, who could help guide them in supporting their spouse or their partner. And also by being there and allowing them to kind of take breaks when the emotional intensity of labor was getting to them. And made them feel okay that they could take care of themselves and not feel like they were abandoning their partner because they’re human too. This is new for them. So yeah, a lot of fathers.
And the research about doulas and their impact on labor companions really feel that they benefit from having another person there. It’s a source of knowledge, information, advocacy, and reassurance. Doulas are also really important for people who are choosing to be single parents, as well as for birthing people who are unable to have their partner or their labor companion of choice present. In EBB Podcast 114, we spoke to a solo parent about her birth story and the role that her doula played for her. And in a more recent episode, episode 303, a military spouse shared about how her doula supported her while her partner was deployed. So sometimes things happen. You can be in a situation where your chosen birth companion just isn’t available, or you could be choosing to enter parenthood solo. And a doula can be a really important source of reassurance for, of course, the birthing person, but also for members of their community, their family, their friends, who will feel confident and feel assured that this person is getting the support they need in the context of the situation in which they’re having their child.
Dr. Rebecca Dekker – 00:31:40:
Yeah, so important. I think doulas play a really critical role around the world, helping ensure that these kinds of parents hopefully don’t birth alone. So super important role that they’re doing. Sara, what about nurses? So you’ve talked about how having a doula is different than a partner’s presence. How is having a doula different from having a labor and delivery nurse with you?
Sara Ailshire – 00:32:05:
Absolutely. So the primary task of a labor and delivery nurse is to provide clinical care, right? They are licensed medical professionals. They can do medical procedures. They have that medical expertise. They form part of your medical care team along with a midwife or with an OB, right? That doesn’t mean that they don’t provide labor support. A lot of labor and delivery nurses do. However, labor and delivery nurses are doing a lot more than just hanging out with one person throughout their entire labor and birth. They have to take care of other patients. They have other responsibilities while they’re on shift. And they can’t sit there and spend the entire time that you’re in labor in the room with you, depending on when you go into labor and if you’re giving birth in the hospital. When you arrive at the delivery ward, you might be there for a shift change or two shift changes. So that means you’ll have maybe more than one team of labor and delivery nurses providing you with clinical care. Nurses are hospital employees. And so while they definitely do fulfill patient advocacy roles, they also have other things that are important and necessary to them. They have to satisfy their employer. They have to be mindful about what their colleagues need, what their team’s interests are.
So in contrast, the primary responsibility of an independent doula, so a doula who’s not employed by a hospital, is their client, is a person who’s giving birth. The doula is there for you and your birthing companion during labor and childbirth. They won’t need to leave the room and go to see another birthing person because they’re going to be there with you throughout this process. They’re not going to need to leave the room for long stretches of time to do charting or to get ready for a shift change to give the other incoming doula a heads up because there’s not typically going to be one. Their primary focus is just supporting you during labor and birth. So I’ve said all of these things about the differences. And while the roles of a doula and a labor nurse are very distinct from one another, something that’s really important to remember is that labor delivery nurses and doulas are typically united in the goal of enhancing people’s health and well-being during birth. Despite having this sort of shared goal, broadly, there can be friction. And this can happen if nurses aren’t sure about what a doula is. If they don’t know about the type of support that a person would like to receive from their doula versus from the labor and delivery nurses. Sometimes nurses might feel that a doula is overstepping. This could be a correct or incorrect assessment. And they could be, maybe, feel frustrated, like, oh, this doula is going to interfere with me being able to do my nursing care.
So there’s some places where friction can arise, but in general, labor and delivery nurses have a lot of experience with doulas. And a lot of labor and delivery nurses, this is just both anecdotal, but also demonstrated in the research, have really positive attitudes towards doulas. And they really value what they bring to the birth room, what they bring to this general team of people who are trying to support a person through birth, each bringing their skillset, each bringing, you know, their knowledge, their expertise, and their particular role, you know, to play here. So educating health workers about what doulas are, what they do, facilitating clear communication and clear expectations around who’s going to be doing what. Can help reduce potential sources of conflict and promote better teamwork between doulas and nurses. In general though, ideally everybody’s on the same team, right? They’re working towards the same goal, which is helping people give birth in a safe manner where their needs embody autonomy are respected and cared for. So that’s a place where I think doulas and nurses have a lot in common. And so while they are distinct roles and there’s lots of differences between the two, that’s, you know, I think a common goal, a common belief that’s shared between these types of professionals.
Dr. Rebecca Dekker – 00:36:20:
And I think it’s improved since I started EBB 12 years ago in 2012. At the time, I think most doulas felt like they were not respected, that they were seen as a nuisance. And in the past decade, at least in the United States and some parts of the country, I’ve seen a huge improvement, anecdotally, of doulas feeling better and nurses feeling better about the whole doula-nurse relationship and partnership. But there are parts of the world where doulas still very much are on the fringes, on the margins. They are looked down upon. They are seen as a nuisance because they’re interfering with the quick, efficient ways of caring for patients that a hospital has decided. And doulas can get in the way in terms of they could stand between you and obstetric violence occasionally. Not always are able to do that, but sometimes they can or do. And in those situations in a hospital where it’s not labeled as obstetric violence, it’s just this is how we do things. So I think there’s definitely much like globally. And we talk more about obstetric violence in the article. So go to ebbirth.com/doulas and you can read the section about the doula’s role in preventing obstetric violence and kind of the complexities and intricacies with that. So I just want to point out that it’s very much location dependent, you know, depends where you live in terms of how doulas are perceived.
Sara Ailshire – 00:37:50:
Absolutely. I think that’s really important to emphasize. So, you know, yeah, depending on your area, if there’s a lot of doulas, nurses, doctors at your local hospital might be very familiar with them. But if you’re in a place where like there might be the only doula in the entire state or the entire region, or maybe even one of a handful in the entire country, it can be a very different experience for sure. So another question I had for you, Rebecca, was why are doulas so effective? Like, is there a way of kind of bringing all of these ideas together that helps explain, why this is?
Dr. Rebecca Dekker – 00:38:28:
Yeah, so when I first drafted this article more than a decade ago, my brain was really turning the wheels in my head because I was like, how do doulas lead to lower C-section rates and better APGAR scores for babies? Like what exactly is going on? So I kind of sketched out what I call a conceptual framework, which is something that researchers use when we’re trying to understand how something is happening. And so you can find that in the article. It’s a graphic. It’s something that we give people permission to use all the time in other materials. And it’s called The Doula Conceptual Framework by Evidence Based Birth®. And so you have the continuous labor support, which we’ve already described. I’m going to tell you some of the things that having this continuous labor support from a Doula does.
One of the things we haven’t mentioned yet is it increases your own natural oxytocin. Oxytocin is sometimes called the love hormone. It’s also the hormone that helps facilitate labor contractions. So there is research that shows that the presence of a doula, their care, their concern, their eye contact, your self-esteem, they help decrease your pain, and they help decrease your anxiety. So all of these things can help shorten labor. They decrease your need for pain medication. So you’re having fewer interventions that can slow down labor as well. And as a result, you don’t need extra interventions to speed up labor. You’re less likely to need Pitocin, for example, because you’re less likely to need an epidural and because you’re moving around and you have higher oxytocin levels. So there’s all of these things that kind of combine together to lead to a decreased risk of Cesarean, better outcomes for the baby because labor has gone more smoothly and with less interventions.
And in the end, you have higher satisfaction as well, not only because of all of these medical factors, but because you felt cared for the whole time. So I think it’s really interesting. You know, we talk about sometimes people think the word intervention has bad connotations, but in the world of research and intervention just means you are intervening. And in this case, we are intervening by putting a skilled, trained person there to care for you and to center your needs, who also has a lot of knowledge about the process of birth? And I think it’s really cool that it’s such a complex thing. Like a human being can be an intervention. You know, you bring this one person onto your team and they do all of these things to influence your birth. I just, I just think it’s incredible. And I have so much respect for the doulas out there who do this work. It’s not an easy job and they bring them their whole selves to these births. They really are using their self as a therapeutic intervention, which is just really cool how human beings can be so effective.
Sara Ailshire – 00:41:59:
No, it’s amazing. And again, I think this speaks while it changes through time. You know, humans have just a long history of supporting each other in birth and we do it cross-culturally and cross time. And maybe we come up with new ways or different labels for it. But I always really appreciate that, you know, it kind of puts us it connects us together in such a important way and we can appreciate it in all these different contexts including appreciating it through a research lens and seeing what we know this feels good but like how what is it going on. So it’s really cool that we can experience these benefits and experience knowing about them all across the board.
Dr. Rebecca Dekker – 00:42:43:
Yeah. And I think for so long, people didn’t understand the importance of labor support and the complexities of what a doula or labor companion can bring to birth. So hopefully this article can continue to shed light on the importance of meeting these needs. And I was curious, Sara, is there any other new research findings you want to highlight about the benefits of doulas or the roles that they play?
Sara Ailshire – 00:43:09:
Yeah, absolutely. So as we were digging into the more recent research, because there hasn’t been a big, like, you know, randomized controlled trial or like Cochrane review in a while, we had an opportunity to kind of take a look at like, different more recent research around the benefits of doulas, particularly for supporting birthing people of color in the LGBTQ plus community.
So one study that we looked at was a 2022 analysis of responses from the 2018 Listening to Mothers in California survey. And these researchers looked at nearly 2,000 responses from women who took part of this 2018 survey. And he found that women of color, as well as women who received Medi-Cal insurance, who reported having a doula present with them during birth, were more likely to report experiencing respectful care during labor and childbirth compared to those who did not have a doula present. And it underscores the importance of having doulas who can relate to the lived experience, the whole person who’s giving birth. So maybe someone who shares the same racial identity as you, who speaks your language, who comes from the same community. Their presence is vitally important. They can understand and connect with you, your needs, your concerns, particularly in a context where obstetric racism can have these sort of negative downstream consequences for the health and well-being of birthing people of color. It’s just really vitally important to have doulas who can connect to people across all different axes of identity. And the research really supports that.
And we were able to cite a number of different studies. And that was a really exciting thing to include in this update. And the other thing that we got to do was talk a little bit more about the experiences of birthing people who are members of the LGBTQI+ community. So lesbian, gay, bisexual, trans, queer, intersex. Because this is a community of people who may have unique pathways into pregnancy and childbirth and have unique needs during birth and postpartum care. So all health providers and all birth workers, including doulas, need to and should be educating themselves about how to best support LGBTQI+ and queer and gender diverse families in pregnancy and childbirth. It was exciting for us to be able to highlight the work that some doula training organizations are doing in providing this education and providing this grounding for birth professionals. And I think we were able to highlight the work of birthing advocacy doula trainings because they’re trying to promote a really inclusive approach to doula support and childbirth and to create trainings that, you know, help address the needs of diverse families. In addition to, and there’s just a couple other different studies that were really interesting about different communities of birthing people and their use of things like birth centers, doulas, midwives that we were able to include. There needs to be more research for sure, but it was nice to be able to introduce this element as well.
Finally, one more thing we were able to add to our article, and it’s something that’s really close to my heart, is to look at global issues that are faced by doulas. Because there’s doulas who are active across the world. And while the research hasn’t always kept up with what doulas are doing in different countries and different communities, we wanted to just highlight the work that’s being done, how doulas are transforming birth care in a variety of settings, how doulas in different countries are kind of transforming what it means to be a doula in particular cultural and social contexts. And how they’re, you know, through that work, they’re transforming how people are giving birth. And at the end of our article, we included some resources about how to find a doula, as well as links to EBB podcasts with doulas practicing outside of, or just practicing all around the world.
Dr. Rebecca Dekker – 00:47:18:
Yeah, I think that that is something the reviewers have told us as well, that one of the main changes to this article is it has more of a global perspective. So we’re really excited that you and Ihotu contributed to that. And another thing you contributed, Sara, is you thought it would be helpful to have a table about guidelines from medical and midwifery organizations and whether or not they support doula presence. So can you talk about that?
Sara Ailshire – 00:47:45:
Yeah, absolutely. You know, I think it’s really interesting to consider. For those of us who are giving birth in hospital-based settings, what are the professional guidelines that might be the basis for the types of care we’re receiving or the types of training that some of our providers are getting. So for this article, we looked at recommendations from the American College of Obstetricians and Gynecologists in the United States, the American College of Nurse Midwives, National Institute for Health and Care Excellence in the UK, and the Royal Australian and New Zealand College of Obstetricians and Gynecologists. All four of these professional bodies recommend that birthing people have birth companions of their choice present at birth. And three of them, the two in the United States, ACOG and ACNM, as well as the National Institute for Health and Care Excellence in the UK, in particular recognized doulas as providing a known benefit to birthing people and were supportive of their presence in birthing spaces because of the benefits they can confer for people who are giving birth. In updating the article, we’ve really built on a strong foundation and we’ve been able to talk about a lot of those changes. But Rebecca, what is the bottom line about the evidence on doulas?
Dr. Rebecca Dekker – 00:49:08:
Great question. I love a good bottom line. My first bottom line is go to ebbirth.com/doulas and download the one-page handout because it has a really nice one-page summary of all this evidence. In more detail, I want to say that evidence shows that continuous labor support is one of the most important and basic and foundational needs of birthing families. And evidence clearly shows that a doula’s presence can improve birth outcomes. It lowers the chances of needing a Cesarean. Doula is lower than need that you may have for medications for pain relief. And they can lower the risk of newborns experiencing a low five-minute APGAR score. Doulas also improve your satisfaction with birth. And they provide an important source, a physical, emotional, informational, and advocacy support for both the birthing person and their chosen birth partners. Doulas are not clinical professionals, but their value in making childbirth safer and more supported has been recognized by leading medical professional organizations, as you mentioned. Research has not shown any medical risks to having a Doula.
However, I do have a quick caveat to that. There may be some potential drawbacks, which we discuss more in depth in the article, if the birthing person has expectatiocens of advocacy that their Doula is not able to fulfill. So, go to the article to learn more about advocacy expectations. In addition, when working with any professional in any field, there is a risk that the person you hire might not fulfill their obligations to you or might not be the right fit for you and your family. Doulas are a diverse group. They have a wide range of perspectives on skills and approaches to birth. And not every doula is the best fit for every birthing family. And we encourage people to meet with several before you decide on the final person, if possible. Likewise, Doulas may decline to work with a client who has expectations that they cannot fulfill, who behaves towards them in an inappropriate manner, or who is dishonest to them. So before any doula or client signs an agreement, we believe it’s important for them both to have gone over their expectations and approaches to birth and have a mutual understanding and communication.
We also know that Doulas are trained to provide support during labor, but they actually do so much more. They engage in wide range of forms of care and support. Some Doulas care for people during the conception journey, through abortions, during and after miscarriage, in the weeks after childbirth, and at the end stages of life. And there’s so many different kinds of training, certifications, traditions, perspectives on doula care. Research has really confirmed what we already knew and what a lot of families know. Doulas can make a big difference in your birth experience, but having a doula is not a magic want. So doulas often work in broken healthcare systems, in the face of oppression, racism, homophobia, transphobia, and other isms. And doulas need all of us to support them in advocating publicly for safer, more supportive birth settings. The doula’s role can also be made more difficult if you and your birth partner have limited knowledge about birth options when you go into labor. So educating yourself about birth as much as possible beforehand can really help equip you with skills that can be combined with the doula’s support.
We know we have people who listen to this podcast who are thinking about becoming a doula. If that is you, it’s important to consider what types of training you want to pursue and what your own approach to birth work may be. And it’s also important to recognize that this can be a demanding field where you may be exposed to challenging situations and traumatic births. So seeking out community support from other doulas can help you process difficult emotions and avoid burnout. But in conclusion, we believe that the evidence shows that doulas provide important benefits for clients, birthing families, entire communities, as well as for hospitals and medical systems. Therefore, doulas should be viewed and valued both by parents and providers as valuable evidence-based members of the birth care team. So that wraps up the article. I did want to let you know again that you can go to ebbirth.com slash doulas to learn more, get more in-depth info about all these topics we covered today. Look at our list of resources. We have tons of lists for you, lists of different interviews, lists of interview questions, that one-page handout that’s really helpful to download all of the scientific references. We link to them at the bottom of the article. And there’s a list of directories as well to find doulas. So overall, we hope that you get a lot of help out of this information being published and that you share it widely so that more people can also learn about the benefits of doulas. Sara, any final words from you?
Sara Ailshire – 00:54:23:
No, it was just a really, I always enjoy contributing to the Signature Articles and getting to do the deep dive into the research. And, you know, really it was fun working with you and with Ahotu on this article. And yeah, I just, I owe a lot personally, professionally to the different types of care that I’ve received from doulas, even, you know, as a researcher. And it was really gratifying to be able to use the research, use the evidence to talk about, you know, the importance of the work that they do.
Dr. Rebecca Dekker – 00:54:54:
Yeah. If you’re listening to this and you’re a doula, we appreciate you and you are valued. You are evidence-based. Hopefully you already knew that, but it’s sometimes nice to have that affirmation of like, yes. You are doing great work. So thanks everyone for listening and we’ll see you next week. Bye. Bye. Today’s podcast was brought to you by the Evidence Based Birth® Professional Membership. The free articles and podcasts we provide to the public are supported by our professional membership program at Evidence Based Birth®. Our members are professionals in the childbirth field who are committed to being change agents in their community. Professional members at EBB get access to continuing education courses with up to 23 contact hours, live monthly training sessions, an exclusive library of printer-friendly PDFs to share with your clients, and a supportive community for asking questions and sharing challenges, struggles, and success stories. We offer monthly and annual plans, as well as scholarships for students and for people of color. To learn more, visit ebbirth.com/membership.
Where does the term doula come from?
Birth companions have been present in all cultures and time periods. In recognition of this, U.S. anthropologist Dr. Dana Raphael used the term “doula” to describe labor companions in her 1966 doctoral dissertation. Later, she expanded and popularized this concept in her 1973 book The Tender Gift: Breastfeeding. Here is an excerpt where Dr. Raphael explains her concept of doula work:
“We have adopted a word to describe the person who performs this function–the doula. The word comes from the Greek, and in Aristotle’s time meant ‘slave.’ Later it came to describe a woman who goes into the home and assists a newly delivered mother by cooking for her, helping with the other children, holding the baby, and so forth. She might be a neighbor, a relative, or a friend, and she performs her task voluntarily and on a temporary basis. It is in the latter context that we use the term “doula” as a title for those individuals who surround, interact with, and aid the mother at any time within the perinatal period, which includes pregnancy, birth, and lactation. The function of the doula varies in different cultures from a little help here and there to complete succoring [aiding], including bathing, cooking, carrying, and feeding. Whatever the doula does, however, is less important than the fact that she is there. Her very presence gives the mother a better chance of remaining calm and nursing her baby. … We might add that the doula, though most frequently female, experienced, and often older, can also be a man. Though inexperienced and young, he may possess the critical ingredients to make the difference–a willingness and ability to be supportive.” (Raphael 1973: 24)
Doulas today continue this legacy of companionship and support. The use of the word “doula” is newer, but the concept of birth work–and of being present for fellow community members in birth–is a longstanding shared cultural practice, rooted deep in human histories.
Note from EBB: Terminology
In this article we use the term “doula” as it is the most widely used word to describe birth companionship and support. However, there are other words that may be used for this role. You may also see the term birthworker, labor support, birth coach, birth sister, perinatal community health worker (a broader term that includes health promotion and education for a variety of perinatal health needs), or community health worker, among others.
Some birth workers dislike the word doula because of its history of meaning “slave” or “servant.” Others feel that it does not address the whole of their work, or that other words might make more sense to their communities. So, while we use the term “doula” throughout this article, and while we focus on the research on doulas, please note that birth companionship does not begin or end with this terminology.
In some locations, a traditional birth attendant or traditional midwife provides birth companionship and (in contrast to a typical doula) will also attend births to “catch babies.” These birth attendants fulfill a cultural midwifery role but may or may not have legal status within their state or country as “licensed” or “certified” midwives (Bohren et al. 2019b; Garces et al. 2019). Traditional birth attendants continue the ancient tradition of a birthing person being supported in labor by family members who have given birth previously, or by a member of the community who has attended many births and developed an expertise through practice.
Note from EBB: History of racism in doula work
EBB recognizes that the late 20th century movement to train and certify doulas was initially led by white doula trainers and doctors who worked to “professionalize” the practice of birth companionship. Although they and their trainees went on to support many families in labor, there were troubling inequities within this movement that went unacknowledged for many years.
The contemporary doula movement owes a great deal to cultures and communities outside the global north. After white men and women in North America learned and “re-discovered” birth practices, in some cases from Indigenous communities and communities of color who never stopped practicing them, they adapted the labor companion role to fit a white consumer model. Doula training organizations in the U.S. and Canada created certifications and training programs, and they claimed authority in the field worldwide. However, other than a few articles, the debt of knowledge and experience that North American doulas owe to dozens of traditional cultures is largely missing from doula trainings and popular books about the field.
Moreover, for many years, white-led doula organizations did not recognize or address their own racism and internal sense of superiority. They also failed to realize how the role of birth companionship would fundamentally change when it became a paid (or reimbursed) position that requires formal training, certification, and re-certification, rather than a voluntary service offered by a trusted community member. These problems in doula work – pervasive implicit bias and a sense of white superiority, a lack of cross-cultural acknowledgment and collaboration, and the commercialization of cultural practices that are then sold by white “experts” back to the communities that preserved them—need to be acknowledged.
Today, there are many programs that train and certify doulas, and a growing number of doula training organizations are led by people of color. Some traditionally white-led doula organizations have taken steps to address racism, credit their original teachers, and promote cross-race collaboration, diversity, equity, and inclusion within their organizations, but the work is ongoing. It is important to understand these historic patterns of inequality, so that we take extra care, and history does not continue to repeat itself.
During the official global launch of Black Doula Day™ in 2024, Black-led doula and birth organizations (Jamaa Birth Village, Black Mamas Matter Alliance, Ancient Song, Atlanta Doula Collective, STL Doulas of Color Collective, Southern Birth Justice Network, Sankofa Healing Center and ROOTT) came together to highlight 7 core demands to “protect, advance, and uplift the Black Doula profession.” Included among these demands are a request for recognition that doulas should not be exploited as a bandage for a broken system. It is crucial that Black, Indigenous, and doulas of color are sought after for their insights and centered by policy makers in the process of drafting legislation about doula care, that they are compensated equitably, and that states should not limit the types of trainings that doulas can take or be certified with. Learn more at https://blackdouladay.com.
Types of doulas
In the late 1900s and early 2000s, the “typical” North American birth doula provided two to three prenatal visits, continuous support during labor/birth, and one visit postpartum. However, in recent years, different types of doulas have emerged and grown in popularity, including postpartum doulas, community-based doulas, full spectrum doulas, and end-of-life doulas. For more information about different types of doulas beyond what is included here, you can check out this link.
Community-based doulas are known, trusted, and skilled individuals who are often from the same marginalized communities as their clients. These special doulas are trained to bridge language and cultural barriers and provide culturally grounded, full-spectrum, and intensive support through pre- conception, pregnancy, postpartum, and beyond (Arcara et al. 2023; LaMancuso, Goldman, & Nothnagle 2016; Health Connect One). They hold important roles as patient advocates who offer emotional and informational support. And they prepare, protect, and hold space for birthing people who are more likely to experience interpersonal and systemic racism through their birthing process (Bey et al. 2019).
Community-based doulas often develop close relationships with their clients. They screen for food insecurity, intimate partner violence, and medical risk factors. They connect families with additional support and care and offer wrap-around care for months or even years later. Learn more about community-based doulas in our Signature Article on Anti-Racism in Healthcare and Birth Work.
Postpartum doulas provide sustained support to birthing people following birth. In comparison to birth doulas, who may offer one or two visits in the early postpartum period, postpartum doulas provide support in the first months after birth. They provide families with support and information about feeding, soothing, and caring for a new infant, as well as offer practical support to family members as they transition into new roles as parents and siblings (Campbell-Voytal et al. 2011; Gjerdingen et al. 2013). Some postpartum doulas also provide care to new families by assisting with light household tasks or night duties related to parenting and infant care.
Full-spectrum doulas offer support before, during, and after pregnancy, including providing support during and after an abortion or loss (Lindsey et al. 2023). Full-spectrum doulas are skilled at providing information and emotional support to people during the full spectrum of pregnancy, from pre-conception, to birth, to abortion, to miscarriage or stillbirth, to adoption, to postpartum (BADT 2021).
End-of-life doulas (also known as death doulas) are companions who support a person towards the end of their life and support the client’s friends and family as they witness the dying process (Krawczyk et al. 2023; Rawlings et al. 2019). Like other doulas, end-of-life doulas are not medical professionals; however, they have experience collaborating with members of their client’s medical or hospice team.
Some doulas, known as loss or bereavement doulas, specialize in providing support to childbearing families who experience miscarriage, fatal fetal diagnosis, stillbirth, or infant loss. In EBB Podcast Episode 195 we speak with a full spectrum doula who focuses on pregnancy and infant loss.
How does someone become a birth doula?
Birth doulas are not medical professionals, and there is no single certifying body that regulates all doulas, standardizes their training, or offers an authoritative certification. Note: For practical purposes, for the rest of this article when we use the term ‘doula’ we are referring to doulas who include birth support in their services. Many doulas choose to be trained and/or certified by independent doula training organizations, but formal training and certification is not a requirement for someone to work as a doula, call themselves a doula, or to provide support during labor and childbirth.
The format of doula training varies widely, from a 3-day in-person workshop with no ongoing mentorship, to a 1-year hybrid in-person and online training with mentorship — and everything in between! Full-spectrum or community-based doula programs tend to offer longer trainings as their trainees go on to offer broader services that cover pre-conception, pregnancy, pregnancy loss, birth, postpartum, and parenting.
There are many doula trainers and training organizations, each with their own area of specialty. Some train internationally, while others choose to focus on a particular country or region. Some certifying organizations offer religious trainings to bring faith practices into the birth experience. Other trainings are tailored to doulas and birthing people who share a racial, ethnic, or LGBTQ+ identity and may want to bring in certain cultural practices, a shared understanding about family, or to protect against misunderstandings or microaggressions from other providers during the birth. Each training organization has a different process for potential doulas to complete and may have different requirements before a doula can be certified with their organization. Some doula training organizations do not believe in certification or re-certification because certification is perceived as inappropriate regulatory control over a voluntary cultural and ancestral community practice.
As a result of this varied landscape of doula organizations, doula trainers, philosophies about doula work and doula certifications, it is common for some doulas to be certified by multiple organizations or trained in multiple types of support.
If you are thinking about becoming a doula, you may want to learn about different doula organizations before deciding which one is the best fit. It is important to consider what types of communities or families you wish to serve, what types of training you want to pursue, and what your own approach to birth work will be.
If you are interested in hiring a doula, you may want to ask your potential doula about their training and/or certification organizations, as part of figuring out what type of doula might be the best fit for your needs.
How many people use doulas?
We have very little data on the number of people who use doulas. In a 2012 survey that took place in the U.S., about 6% of birthing people said they used a doula during childbirth (Declercq et al. 2013), up from 3% in a 2006 national survey (Declercq et al. 2007). Of those who did not have a doula but understood what they were, 27% would have liked to have a doula.
In a 2018 survey that took place in California, 9% of birthing people said that they used a doula during childbirth. Rates of having a doula were higher among Latina women (10%), and Black women (15%) (Sakala et al. 2018).
There is limited research on this topic so far, but families may encounter several barriers to having a doula, including:
- The cost of paying a private doula.
- Being ineligible for and unaware of possible free doula programs in your area.
- The time it takes to interview and find a doula you connect with.
- Learning about doulas too late in your pregnancy, or after the birth.
- Being unaware of the many different types of doulas.
- Thinking that partners, midwives, nurses, or friends can offer the same support as doulas.
- Doulas are not allowed at your hospital or birthing location.
- Your birthing location has policies limiting the number of people who can attend your birth (meaning you have to choose between a doula and other family members or friends).
- Beliefs that doulas are “nice to have,” but only for the wealthy or the very disadvantaged.
What do doulas do?
Doulas nurture and support you during pregnancy, labor, birth, and the postpartum period. They provide continuous support through labor and birth. They bring a non-medical approach that focuses on providing emotional and physical support, sharing information, and helping prepare you and your support system prior to birth. They typically have stronger labor support and relational skills than most medical staff or health care workers.
It’s quite common that the first time you meet the nurses, midwives, and doctors who assist you in birth will be during the labor or birth itself. By contrast, most doulas aim to establish a relationship with you and your birth partner(s) before the birth—and research shows that families feel more secure going into labor with a doula they already know and trust (Banda et al. 2010; Akhavan & Lundgren 2012; Lunda, Minnie, & Benadé 2018). Doulas find that this mutual trust is important for providing effective support in labor (Bohren et al. 2019a).
Also, many families are surprised to find that medical providers do not stay with you for very long during labor—instead, they do brief check-ins, with a focus on carrying out medical tasks. This is quite different from doulas, who usually stay with you from the beginning to the end of labor. We explore the evidence on the benefits of continuous support of doulas in childbirth later in this article.
Some doulas, such as community-based doulas, have expanded roles where they support you throughout your pregnancy. And there are postpartum doulas who provide extended care after the birth for newborn feeding and parenting support.
Many doulas may offer other services or forms of expertise in addition to being a doula. From placenta encapsulation to birth photography to lactation support, many doulas are multi-hyphenated birth workers.
On top of building trust with you, a doula’s essential role is to support you through labor and birth, no matter what decisions you make or how you choose to give birth.
What is labor support?
Labor support is defined as the therapeutic presence (human-to-human interaction with caring behaviors) of another person with you during labor (Jordan 2016).
Labor support is typically provided in-person, but sometimes it is provided virtually. During the first years of the COVID-19 pandemic, hospital restrictions meant that some doulas could not accompany their clients into hospitals to provide in-person labor support. Doulas found creative ways to provide virtual labor support, often staying on the phone with birthing people and remaining in contact throughout labor and birth, or by providing postpartum support via video call, or dropping off supplies to new parents (Ochapa et al. 2023; Oparah et al. 2021).
Any person who is on your care team (such as a family member or friend, nurse, student, midwife, and even the occasional physician) can provide labor support. However, doulas are unique in that their entire focus is continuous labor support—they do not have other clinical tasks distracting them from this role. The benefit of continuous labor support is so powerful that researchers have found that providing even brief doula training to friends and family members can improve birthing people’s experiences in childbirth (Nguyen & Heelan-Fancher 2022).
The doula’s role and goals are tied solely to your goals. This is known as primacy of interest. In other words, a doula’s primary responsibility is to the birthing person — not to a hospital administrator who may be thinking about finances, not to a charge nurse who may be worrying about bed availability, not to a partner who may be wrestling with their own anxieties, and not to the midwife or doctor who may be concerned about avoiding rare life-threatening emergencies or protecting their own legal liability.
The four pillars of labor support that a doula can provide include physical support, emotional support, informational support, and advocacy.
Physical Support
“We called our doula and she was at the hospital waiting for us. She was there when I got out of the car, and she and Henry [partner] were holding me through contractions as we made our way into the hospital. I have a very vivid memory of her holding my shoulder and then slowly moving her hand down my arm as my contractions faded. It made me feel more relaxed as the contractions ended and then Henry started doing something similar. It was amazing, at times I didn’t know whether it was her or Henry, but I remember that feeling so, just very caring.” (Hunter 2012)
Feeling physically and emotionally safe during childbirth is important to ensure the best outcomes (Kozhimannil et al. 2016). Physical support is important because it helps you maintain a sense of control, comfort, and confidence, and can provide relief or distraction from pain. Feeling safe can also calm your nerves and allow your body to stay in a relaxed state, so labor will progress at its best. Some examples of physical support that doulas can provide include:
- Soothing touch with massage, counter pressure, acupressure, or other techniques.
- Creating a calm environment, such as dimming lights and arranging curtains.
- Assisting with water therapy (shower, tub).
- Applying warm or cold packs.
- Holding hands and making eye contact.
- Teaching breathing and visualization techniques.
- Guiding you with positions, movement, swaying, pelvic rocking, or using a birth ball or peanut ball.
- Assisting you in walking to and from the bathroom or changing clothes.
- Giving ice chips, food, and drinks.
In low-resource settings or hospitals with staff shortages, doulas can also provide practical support by filling in gaps in care (Khaw et al. 2022). This can include:
- Offering interpretation support or culturally competent care.
- Alerting the staff about unusual symptoms or issues in labor.
- Enhancing continuity of care.
- Changing bedding or maintaining the hygiene and cleanliness of the room.
Community-based doulas may provide even more forms of physical support, such as attending prenatal appointments with you, helping you access nutritious foods, and hosting more frequent in-person or virtual meetings (Arcara et al. 2023; Cidro et al. 2021; Ireland, Montgomery-Andersen, & Geraghty 2019; Wint et al. 2019).
Emotional Support
“With the help of the doula I can trust my ability… she praised me when she heard how I handled my contractions; I could trust that I was on my way into the next stage. It was like an affirmation.” (Berg & Terstad 2006)
Emotional support is a key feature of doula support, helping you feel cared for and centered in your care, and to feel a sense of pride and empowerment after birth. One of the doula’s primary roles is to care for your emotional health and provide a supportive presence that increases the chances of a positive birth experience (Gilliland 2010b).
Doulas may provide the following types of emotional support to you and your birth partner(s):
- Continuous presence.
- Reassurance.
- Encouragement.
- Praise.
- Helping you see yourself or your situation more positively.
- Helping you feel more in control and confident, and aware of your progress.
- Keeping company.
- Showing a caring attitude.
- Calmly describing what you’re experiencing and echoing back the same feelings and intensity, or by mirroring facial expressions.
- Accepting what you and your family want.
- Showing sensitivity to you and your family’s emotions, and helping you work through fears and self-doubt.
- Spiritual support if requested, such as sharing prayers or reading from inspirational texts.
- Debriefing after the birth—listening with empathy.
Informational Support
“[My doulas] gave me another packet of information of things I should be eating… Like preterm labor signs that I should be looking out for… and then things like optional versus protocol in a hospital setting. Like when I’m in labor. Just things that I didn’t even think about or know about.” (Arteaga et al. 2023)
Informational support helps keep you and your birth partner(s) informed about what’s going on with the course of labor, as well as giving you evidence-based information about birth options. All of this can lead to you feeling supported, safe, and experiencing other benefits that come from being at ease in your body. Studies show that doulas often have a basic level of clinical knowledge and can help explain the birthing process and common medical procedures (Bohren et al. 2019b).
Informational support can include:
- Educating you or your family about the birthing process, how long to expect each phase of labor to last, and reasons why medical staff may propose medical interventions.
- Suggesting techniques in labor, such as breathing, relaxation techniques, movement, and positioning (positioning is important both with and without epidurals).
- Helping you find evidence-based information about different options in pregnancy and childbirth.
- Helping explain medical procedures before or while they occur.
- Helping your birth partner(s) understand what’s going on with your labor (for example, interpreting the different sounds you might make).
- Assisting with communication between you and medical providers about medical decisions or procedures – making sure that you and your birth partner(s) understand medical terms and have your questions answered, and that the medical team understands your preferences.
- Helping you and/or your birth partner(s) to speak up and be more engaged, rather than confused or anxious.
- Communicating with additional family members or friends who have come to visit to explain what is happening, how they can support, and when is the best time to enter the birth room (or why it may be best to wait).
Informational support is especially important for birthing families who struggle to understand the language or culture of the hospital, experience neglect or discrimination in health care, or are overwhelmed by the challenges of giving birth.
Advocacy
“There’s so many different ways that you can advocate for somebody, and even with the clients that I work with, I feel like advocacy and what they expect from advocacy looks different depending on who they are, their income level, their race, their gender, their sexual identity. All the different things contribute to advocacy but it looks different depending on the person’s lens.” Sabia Wade, Birth Allowed Radio, episode 37.
Advocacy has become an important conversation within doula care, because birth can be a challenging experience on its own, and because families have experienced trauma, lack of consent, or disagreement with some health care providers about medical decisions. Advocacy is a pillar of support of doula care that can take many forms. Key reasons for this include:
- The term advocacy has several meanings and definitions.
- Doulas differ on how and whether advocacy is part of their role.
- Clients may have different preferences about what kind of advocacy they want from their doula.
- Every doula’s unique approach to advocacy will lead them to different ways of interacting or collaborating with medical staff, as potential solutions or workarounds.
In research on the concept of advocacy in the nurse’s role, Kalaitzidis and Jewell (2015) compiled all the existing definitions of patient advocacy. They found that the most common definitions of advocacy were “pleading the cause of someone” or “speaking on behalf of someone.” Advocacy can also be defined as “supporting an individual or group to gain what they need from the system” or supporting a person in their right to self-determination.
Considering the past definitions of advocacy for nurses, here at Evidence Based Birth® we use the following definition of advocacy in the context of doula care:
Advocacy is defined as supporting the birthing person in their right to make decisions about their own body and baby.
Doulas have diverse perspectives about advocacy
Advocacy has long been considered an essential component of the nurse’s role. However, while some doulas believe that advocacy is a part of their role, others have been specifically trained that advocacy is not part of their role at all.
Foundational to doula practice is the philosophy that a birthing person’s autonomy, or a person’s ability to decide for themselves what they want or do not want during childbirth, is paramount. Doulas assist in this process by facilitating communication, making space and time for reflection, and providing informational or decision-making support (Meadow 2014; Rysdam 2019). However, there is a wide range of individual doulas’ advocacy and communication skills, their desire to advocate or not, and how they support client autonomy.
For many years, DONA International, one of the first doula training and certification organizations, stated in their standards of practice that advocacy is part of the doula’s role, but only if the doula does not speak on behalf of the client (DONA 2020). However, many doulas have reported to EBB that their doula trainers (from a variety of established doula training organizations) specifically instructed them not to speak at all to health care providers. Furthermore, many doulas do not want to speak for their client, and they are afraid of being mistakenly perceived by health care workers as making medical decisions for their client (Amram et al. 2014).
However, some doulas take a more active role in speaking up to the medical team about a birthing person’s preferences or needs (Cidro et al. 2021; LaMancuso, Goldman, & Nothnagle 2016; Lunda, Minnie, & Benadé 2018; Ochapa et al. 2023; Oparah et al. 2021; Sayyad et al. 2023; Thomas et al. 2023; Van Eijk et al. 2022). This may be particularly true for doulas who work with birthing people who experience obstetric racism or with families who do not share a common language or culture with their medical providers. These doulas may see their role as assisting their client’s access to higher quality safe care, by making sure that there is clear communication and agreement between the medical team and their patient, and that the patient’s choices, pain, and requests for support are respected and protected.
Some doulas, particularly Black doulas who regularly confront obstetric racism and its potential outcome of mortality, use a wider range of advocacy skills, depending on the unique scenario (Arteaga et al. 2023; Cancelmo 2021; Davis 2022; Salinas, Salinas, & Kahn 2022).
Advocacy techniques doulas may use
The following are some examples of advocacy techniques used by doulas.
Here are some more subtle advocacy techniques:
- Encouraging you or your birth partner(s) to ask questions and speak up about your preferences.
- Asking you what you want.
- Verbally supporting and reminding you of your decisions.
- Creating space and time for you and your birth partner(s) to ask questions, gather evidence-based information, and make decisions without feeling pressured.
- Coaching you and your birth partner(s) on positive communication techniques to use with your medical team. This can include asking canned questions to reinforce knowledge or to gently encourage medical staff to remember a client’s birth plan or birth preferences.
- Facilitating clear communication and a sense of collaboration between you and your care providers.
- If you are not aware that a provider is about to perform an intervention, the doula could point out what it appears the nurse or physician is about to do and ask you if you have any questions about what is about to happen. For example, if it looks like the provider is about to perform an episiotomy without your consent: “Dr. Smith has scissors in her hand. Do you have any questions about what she wants to do with the scissors?”
And here are some more direct advocacy techniques a doula may use:
- Amplifying your voice if you are being dismissed, ignored, or not heard. For example, the doula could say, “Excuse me, [insert client’s name] is trying to tell you something. I wanted to make sure you heard them.”
- Telling a provider to stop if they actively perform an intervention on a client who is refusing. For example, the doula could say, “Stop, she said no to the episiotomy.” Or asking the client “Do you consent to this procedure?”
- Filling communication gaps between family, friends, or visitors and what’s happening in the birthing room (i.e. explaining when they can come in, or why it’s not a good time).
- Asking to speak with a nurse in the hallway and informing them that using specific terms or gestures could be triggering a trauma response in the client that will make their job more challenging down the line, and could have an impact on parent or baby health outcomes.
- Informing the nurse or physician that they need to provide an interpreter to gain informed consent.
- Reminding the care team that you requested no students, so there cannot be a series of students sent into the room to perform repeated cervical exams on you.
- Right before the baby is born, reminding the care team of your wish for delayed cord clamping.
- Alerting the care team to concerning signs or symptoms, such as excessive blood loss or signs of preeclampsia.
Obstetric violence and the limits of advocacy
The term obstetric violence was coined by Latin American activists to describe violence that can occur within the field of obstetrics. Although other terms such as “traumatic birth,” “mistreatment,” “abuse,” and “disrespectful care” are also used, here at EBB we choose to use obstetric violence to describe traumatic events and/or physical or emotional harm caused by prenatal or obstetric health care staff before, during, or after giving birth (van der Waal et al. 2022).
Although parents may hope their doula’s advocacy can help protect them from obstetric violence, the reality is a lot more complicated. Doulas can help you advocate for yourself and may act as a buffer, but ultimately the doula also has to negotiate with strong power dynamics on a hierarchical medical team, where the most educated provider is often seen as the authoritative decision maker.
When selecting a doula, it is important to ask your doula what their beliefs are about advocacy in the birth room. What is their past experience in tough situations? What strategies seemed to work best? They should share with you the approach they take, and which types of advocacy they do and do not provide. Birthing people can also reflect on the type of advocacy support they want from a doula and directly share this information with any doula they are considering working with. When selecting your medical provider or birth center, pay attention during appointments or visits to how your provider communicates with you and how you feel afterwards. This can be an important source of information that you can use to avoid working with a provider who makes you feel unheard, disrespected, or unsafe.
As Cristen Pasccuci, advocate and expert in preventing obstetric violence, states:
“Unfortunately, I’ve had many conversations with mothers who experienced obstetric violence with their doula present and who felt betrayed or even traumatized by what they felt was their doula’s lack of advocacy, as well as conversations with doulas distraught that they could not protect their clients from abusive providers. We have to hold a lot of nuances to talk about this.
Most doulas in the U.S. are constrained in their ability to advocate to the fullest because of power dynamics and systemic realities their clients may not even be aware of, and doulas absolutely cannot prevent all mistreatment in birth—it’s more like harm reduction. And, while many doulas are skilled, experienced advocates, others are not trained in advocacy skills even if they are willing to advocate, and some doulas believe it is not their job to advocate.
So, it’s really important for parents and doulas to have open and transparent conversations about their expectations and plan for what advocacy will actually look like in the birth room.”
Cristen Pascucci, founder of Birth Monopoly
What is not included in doula support?
Doulas are not medical professionals, and in general, the following tasks are not performed by doulas:
- They do not perform clinical tasks such as cervical exams or fetal heart monitoring.
- They do not give medical advice or diagnose conditions.
- They do not make decisions for the client (medical or otherwise).
- They do not pressure the birthing person into certain choices just because that’s what they prefer.
- They do not take over the role of the partner.
- They do not catch the baby.
- They do not typically change shifts (although some doulas may call in their back-up after 12-24 hours; and some volunteer doulas may take assigned shifts).
However, some doulas may also wear another “hat” as a health care professional! It is not uncommon to meet labor and delivery nurses or midwives who have also trained as doulas. Some birth professionals who hold multiple credentials may refer to themselves and offer services as a monitrice. A monitrice is a licensed or certified health professional (such as a labor and delivery nurse, a certified practicing midwife, a certified nurse midwife, etc.) who also offers doula care services. The monitrice has the training and scope to offer services in the home setting such as checking vital signs, monitoring fetal heart tones, or performing a cervical check upon request.
For example, a monitrice might perform a cervical check to confirm that you are in active labor before heading to the hospital. Once at the hospital, they function as a doula (because they are not functioning in a staff nurse or midwife role) but can also share information with their client based on their training and certification as a licensed professional. Most doulas are not monitrices, so if you are interested in this type of care, you will want to seek out someone who is a licensed nurse or midwife, has experience working as a doula, and is comfortable combining their roles in this way.
Can my friend or family member serve as my doula?
A lay doula is a partner, friend, or family member who has attended births informally, or has given birth themselves, but does not have formal training as a doula. Emerging research suggests there are benefits to working with a lay doula!
In 2020, researchers looked at the relationship between having a labor companion present at birth and exposure to mistreatment in childbirth across four countries (Myanmar, Ghana, Guinea, and Nigeria). They found the presence of a labor companion, even one with no formal training in labor support, helped protect birthing people from mistreatment in childbirth (Balde et al. 2020).
In a 2019 Cochrane Review on labor companions during childbirth, researchers reviewed 51 studies, primarily (but not entirely) from high-income countries about self-identified women’s experiences in childbirth (Bohren et al. 2019b). They found that the labor companions positively influence the dynamic between birthing women and health care providers. The presence of labor companions helped protect women from mistreatment in childbirth, and improved outcomes because they noticed and called attention to potential issues throughout labor and birth. The researchers also found that most birthing women in the studies both wanted and benefited from the presence of a labor companion, whether it was a trained professional or a family member, partner, or friend.
In a 2022 systematic review, researchers combined nine studies with nearly 7,000 participants to explore the benefits of female relatives acting as lay doulas (Nguyen & Heelan Fancher 2022). The results showed that birthing people consistently reported positive birth experiences when their female relatives served as lay doulas. However, the lay doulas’ impact on the rate of Cesareans and length of labor was inconsistent – some studies showed a positive impact, while others found no difference. Overall, this review concluded that the positive benefits of continuous labor support were most beneficial when provided by a formally trained doula, who is not part of the hospital staff.
Can my spouse or partner serve as my doula?
“She [the doula] helped him a lot out with getting him ready for when I had the baby, because I don’t think he was going to know what to do. But he was helping me breathe and stuff.” (Thullen et al. 2014)
Some people think that they do not need a doula because their partner will be with them continuously throughout labor. It is true that a birth partner(s) is an essential support person for a birthing person to have by their side. However, the birth partner will need to eat and use the bathroom at times, and they may also need support in their own emotional journey. For example, if your birth companion is becoming a parent for the first time, they may be struggling with a lack of hospital support for them as they transition into a new role (Hodgson et al. 2021; van Vulpen et al. 2021).
Also, many partners have limited knowledge about birth, labor positions, medical procedures, or what goes on in a hospital, while doulas have knowledge and experience about all these things that they can use to inform and support both the partner and birthing person. Ideally, doulas and partners can work together to make up a labor support team.
In one landmark study that evaluated the effects of doulas and fathers working together, researchers found that combining a supportive partner and a doula significantly lowered the risk of Cesarean compared to just having a supportive partner alone. In 2008, McGrath and Kennell randomly assigned 420 first-time birthing women to have routine care (including a supportive partner) or care that also included a professional doula whom they met for the first-time during labor. All the women in the study were classified as having middle- to upper-class financial income levels, having supportive partners, and being in the care of obstetricians.
During labor, doulas provided continuous support, including encouragement, reassurance, and physical support. They helped the partner support the laboring person and were careful to respect the partner’s role.
The results showed a substantial improvement in outcomes for women who had both a birth partner and a doula, compared to having a birth partner alone. The Cesarean rate for these first-time mothers was 25% in the group with a partner only, and 13.4% in the group with a partner and doula. The women who had their labor medically induced experienced an even more striking decrease in the Cesarean rate with a doula—the Cesarean rate with labor inductions was 58.8% in the group without a doula, and 12.5% in the group with a doula. Also, fewer women in the doula group required an epidural (64.7%) compared to those without a doula (76%).
Research has shown that the most positive birth experiences for fathers were ones where they had continuous support by a doula or a midwife. In the McGrath and Kennell study, the women and their partners who had a doula overwhelmingly rated the support of their doula as positive—with 93% rating their experience with the doula as very positive, and 7% as positive.
In other studies, fathers have said that when they had labor support from a midwife or doula, things were explained to them, their questions were answered, their labor support efforts were guided and effective, and they could take breaks from the emotional intensity of the labor without abandoning their laboring partner (Johansson 2015). Doulas can educate partners not only about birth, but also about how to advocate for the birthing person (Ochapa et al. 2023; Oparah et al 2023).
Doulas also provide important support for birthing people who are single parents, as well as for birthing people whose partners are unable to be present during labor and birth. In EBB Podcast 114, we speak with a solo parent about her birth story and the role her doula played in supporting her. And in EBB 303, a military spouse shares how doulas supported her throughout labor while her partner was deployed.
How is a doula different from my labor & delivery nurse?
During hospital births, doulas spend more time with you than other members of the obstetric team, such as nurses (Lucas & Wright 2019). The primary task of a labor and delivery nurse is to provide clinical care. That does not mean that a labor and delivery nurse does not provide any labor support—sometimes they do! However, they also must care for other patients and can only spend a limited amount of time in your room. Labor and delivery nurses are also mentally attending to two patients every time they enter your room: you and the baby (or babies). So, their clinical focus and decision making may sometimes be focused on the fetal monitor and not on you.
In one research study that took place in the U.S., nurses spent about 31% of a person’s labor in the room with them. Most of the time that nurses were in the laboring person’s room, they were doing direct clinical care (such as administering medications or performing interventions), maintaining equipment, applying, and assessing the output from the electronic fetal monitor, or documenting at the computer. For 12% of each person’s labor in the study, the nurse provided labor support including emotional, physical, or informational support, or advocacy. More experienced nurses were more likely to spend time providing emotional support (Barnett et al. 2008).
Three other studies in Canada have found similar findings—that nurses spend about 50-75% of their time outside the birthing person’s room. In addition to caring for their assigned client, nurses have many other responsibilities, like communicating with care providers, taking care of other clients, covering for other nurses’ breaks, documenting care, and assisting on the labor unit as necessary (Gagnon & Waghorn, 1996; McNiven et al. 1992; Gale et al. 2001).
Nurses are employed by the hospital and while they see themselves as patient advocates, they also have an interest in satisfying their employer, doctors, and midwives. By contrast, the primary responsibility of an independent doula (one not employed by the hospital) is to you.
Nurses may also go off shift during your labor, at which point their support ends and another nurse takes over your care. Most doulas, on the other hand, remain with you throughout your labor and birth whether it is long or short. Most will also plan with you about how and when to include a back-up doula in your care, to ensure you receive the continuous care and attention you need.
Both doulas and nurses may touch you at different points during labor. Doulas may use touch to provide counter-pressure, soothe you, help you get into a desired laboring position, or assist with other comfort measures. If you met your doula prior to giving birth, they may have discussed with you what physical support might look like during birth and practiced comfort or support techniques with you ahead of time.
Nurses may also provide physical support during or after labor. They may help you change laboring positions, help you feel clean during labor by changing the bedding, or help you with toileting after birth. What is different is that nurses will also perform medical tasks—such as placing an IV, assisting with inserting a Foley bulb catheter or device, conducting a cervical exam, or putting pressure on your abdomen after the birth. Some of these forms of touch may be unpleasant, and all require consent from the birthing person (but sometimes consent is not obtained). When and how a doula touches is up to the person giving birth, and their touches bring measures of comfort rather than discomfort—so your brain and body are probably trained to respond to the doula more positively over time (Personal communication, A. Gilliland 2017).
While the roles of a doula and of a labor nurse are distinct from one another, they are both united in providing support to enhance your health and wellbeing. Despite this, sometimes friction can arise if nurses are unsure of the role of a doula, or if they don’t know what forms of support the client would prefer to receive from their doula versus from their nurse. Sometimes nurses may believe (accurately or inaccurately) that a doula is overstepping their role and interfering with the nurse’s duties (Ballen & Fulcher 2006; Neel et al. 2019). But many nurses have a positive attitude towards doulas and value what they bring to the birth room (Ballen & Fulcher 2006; Neel et al. 2019).
Educating health care workers about the role of doulas, as well as facilitating clear communication between doulas, birthing people, and nurses about needs and expectations can reduce potential sources of conflict and promote better teamwork between doulas and nurses (Lucas & Wright 2019; Neel et al. 2019; Roth et al. 2016).
What is the evidence on doulas?
Cochrane Review (2017)
In 2017, Bohren et al. published an updated Cochrane review on continuous support in childbirth. They combined the results of 26 trials with more than 15,000 people across 17 countries including North America, South America, Europe, the Middle East, Africa, Asia, and Oceania, in both high-income and middle-income settings.
People in these studies were randomly assigned (like flipping a coin) to either receive continuous, one-on-one support during labor or “usual care.”
The Cochrane reviewers said the overall quality of the evidence was low quality, according to the GRADE system for assessing evidence. An important part of analyzing this study is understanding the reason for the low rating.
In the GRADE system, the quality of evidence for each outcome is rated as high, moderate, low, or very low. A GRADE rating of high would be considered great evidence—and that the authors can be confident that the true effect of doulas is very close to the effect seen in the study results. On the other hand, a rating of very low means that there is little confidence in the findings, and that the true effect of doulas could be very different than what was seen in the study results. The two middle ratings of moderate and low aren’t great, but they aren’t weak, either. In a clinical trial, it’s preferable to hide, mask, or “blind” everyone as to which treatment is being given, to avoid the placebo effect. Since it is not possible to blind participants or care providers as to who has doula support (doulas aren’t invisible!), the quality of the evidence for doulas automatically received a lower grade.
In this review, continuous support was provided either by hospital staff, such as a midwife or nurse (nine studies), doulas who were not part of the family social network and not part of hospital staff (doula, eight studies; childbirth educators, one study, retired nurses, one study), or a companion from the family’s social network, such as a female relative or a partner (seven studies). In 15 studies, the partner was not allowed to be present at birth, and so continuous support was compared to no support at all. In all the other 11 studies, the partner was allowed to be present in addition to the person providing continuous labor support.
Overall, birthing people who received continuous support were more likely to have spontaneous vaginal births and less likely to have any pain medication, epidurals, negative feelings about childbirth, vacuum or forceps-assisted births, and Cesareans. In addition, their labors were shorter by about 40 minutes on average, and their babies were less likely to have low Apgar scores at birth (an Apgar score is a measure of a baby’s immediate health at birth). There was some evidence that doula support in labor lowered rates of postpartum depression. There was no evidence that there are any negative effects of doula support.
The results of this study mean that continuous support, including support from a doula, is a safe and beneficial way to increase the likelihood of better outcomes for the birthing person and the baby.
How did doulas compare to the other types of continuous support?
The Cochrane reviewers also looked to see if the type of support made a difference. They wanted to know—does it matter who provides continuous labor support? Does a midwife, doula, or partner, friend, or relative offer more benefit? The researchers were able to look at this question for six topics: use of any pain medication, use of Pitocin® during labor, spontaneous vaginal birth (a vaginal birth that happens on its own), Cesarean, admission to special care nursery after birth, and negative birth experiences.
For two of the health outcomes below (designated with asterisks*), the best results occurred when a birthing person had continuous labor support from a trained doula– someone who was NOT a staff member at the hospital and NOT part of their social network.
The researchers found that overall, continuous support during birth leads to a:
- 25% decrease in the risk of Cesarean; the largest effect was seen with a doula (39% decrease)*
- 8% increase in the likelihood of a spontaneous vaginal birth; the largest effect was seen with a doula (15% increase)*
- 10% decrease in the use of any medications for pain relief; the type of person providing continuous support did not make a difference
- Shorter labors by 41 minutes on average; there is no data on if the type of person providing continuous support makes a difference
- 38% decrease in the baby’s risk of a low five-minute Apgar score; there is no data on if the type of person providing continuous support makes a difference
- 31% decrease in the risk of being dissatisfied with the birth experience; this risk was reduced with continuous support provided by a doula or someone in their social network (family or friend), but not hospital staff
The rate of special care nursery admissions was no different between people who received continuous support and those who received usual care.
It’s important to note that these decreases in risk are relative risk reductions—which requires you to carry out a math formula to understand the true reduction in risk. Relative risk is the risk of something happening to you in comparison to someone else. Absolute risk is the actual, or true risk of something happening to you.
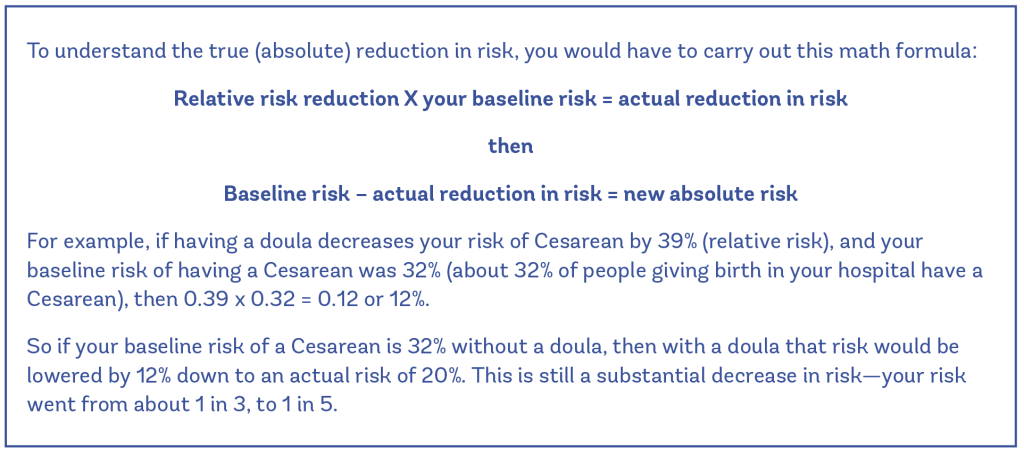
Why are doulas so effective?
There are several reasons why resear
chers think doulas are so effective. The first reason is the “harsh environment” theory. In most countries, ever since birth moved out of the home and into the hospital, people in labor are frequently submitted to institutional routines, high intervention rates, staff who are strangers, lack of privacy, bright lighting, and needles.
Most of us would have a hard time dealing with these conditions when we’re feeling our best, let alone in a vulnerable state and while managing the physical and emotional intensity of labor. These interruptions, distractions, encounters with strangers, an unfamiliar environment, and sometimes painful procedures can slow down labor and chip away at your focus and self-confidence. A doula “buffers” this harsh environment by providing continuous support, helping you to regain your focus, and providing encouragement and trusted companionship which promotes self-esteem (Hofmeyr et al. 1991).
A second reason doulas are effective is because doulas are considered a form of pain relief in themselves (Hofmeyr et al. 1991). With continuous support, you are less likely to request an epidural or pain medication. It is thought that there is less use of medication because many people with a doula feel less pain, are less likely to need an epidural, and may avoid the cascade of medical interventions that often go along with an epidural, including Pitocin® augmentation and continuous electronic fetal monitoring (Caton et al. 2002). Theoretically, the soothing touch of a doula may also help your body pay less attention to pain signals, a phenomenon known as the Gate Control theory of pain relief.
The research result—that people with doulas are less likely to have an epidural—is not due to the fact that clients with doulas in these studies were more likely to want these things up front and were more motivated to achieve them. In fact, randomized trials account for these differences—this is why they are called randomized, controlled trials. The people assigned to have a doula and those assigned to not have a doula are randomly assigned, meaning that the same percentage in each group would be planning a medicated or unmedicated birth.
A third reason why doulas are effective has to do with the attachment between the birthing person and doula which can lead to an increase in oxytocin, the hormone that promotes labor contractions. This theory was proposed by Dr. Amy Gilliland in her 2010(a) study about effective labor support.
In personal correspondence with Dr. Gilliland, she wrote, “I believe the doula effect is related to attachment. When the mother feels vulnerable in labor, she directs attachment behaviors to suitable figures around her, who may or may not be her attachment figures (parent, mate). When the mother directs attachment seeking behaviors to the doula, the experienced doula (25 births or more) responds in a unique manner. She is able to respond as a secure base, thereby soothing the mother’s attachment system. The accompanying diminishment in stress hormones allows for a surge in oxytocin in both the mother and the doula… theoretically, oxytocin is the hormone that promotes labor contractions. This theory was proposed by Dr. Amy Gilliland in her 2010(a) study about effective labor support.
In personal correspondence with Dr. Gilliland, she wrote, “I believe the doula effect is related to attachment. When the mother feels vulnerable in labor, she directs attachment behaviors to suitable figures around her, who may or may not be her attachment figures (parent, mate). When the mother directs attachment seeking behaviors to the doula, the experienced doula (25 births or more) responds in a unique manner. She is able to respond as a secure base, thereby soothing the mother’s attachment system. The accompanying diminishment in stress hormones allows for a surge in oxytocin in both the mother and the doula… theoretically, oxytocin is the hormone of attachment, and it is released during soothing touch and extended eye contact, which are habitual behaviors of birth doulas.” (Personal communication, Dr. Amy Gilliland 2015).
Swedish oxytocin researcher Kristin Uvnas Moberg writes that the doula enhances oxytocin release which decreases stress reactions, fear, and anxiety, and increases contraction strength and effectiveness. In addition, the calming effect of the doula’s presence increases your own natural pain coping hormones (beta-endorphins), making labor feel less painful (Uvnas Moberg 2014).
A study in Iran compared first-time parent’s anxiety and pain levels with doula support to those without doula support (Ravangard et al. 2017). They randomly assigned 150 first-time births to either doula support, or no doula support, and used standard questionnaires to measure anxiety and pain levels. They found that on average, those who received doula support had less anxiety and lower average pain scores during labor. The authors concluded that the doula’s presence has a clinically meaningful impact on anxiety and pain levels in first-time births. They recommend that all hospitals and maternity care centers in Iran provide access to doulas since having a safe and calm delivery is considered a human right.
Based on the evidence, our team at Evidence Based Birth® came up with a conceptual model of how doula support influences outcomes. A conceptual model is what researchers use to try and understand how a phenomenon works. Here is our conceptual model on the phenomenon of doula support:

How can doulas promote equity and protection for Black, Indigenous and people of color?
“The doulas are aware of… systematic racism within healthcare and a lot of people aren’t privy to that. And so, it was just an insurance of like, ‘Hey, we got you. We’ll walk you through everything, and we’ll just make sure that you feel comfortable with everything.’” (Arteaga et al. 2023).
“[Black] Birth workers committed to the tradition of justice work and movement building are not solely helping to navigate a birth. They are part of a rich history of Black activism.” (Davis 2019a)
Researchers have observed that Black, Indigenous, and other people of color are subjected to individual, institutional, and other forms of racism throughout their lives; these experiences build on each other and are uniquely stressful, and the increased stress can negatively impact pregnancy outcomes (Giscombé and Lobel 2005). Experts in racial health disparities, such as Dr. Joia Crear-Perry, OB-GYN, Founder of the National Black Equity Collaborative, often clarify with the explanation:
“Race isn’t the risk factor – racism is.”
Addressing Obstetric Racism
Anthropologist, professor, and doula Dána-Ain Davis developed the term obstetric racism to help explain the impact racism has on Black birthing people.
Davis (2019b) defines obstetric racism as:
“…a threat to maternal life and neonatal outcomes. It includes, but is not limited to, critical lapses in diagnosis; being neglectful, dismissive, or disrespectful; causing pain; and engaging in medical abuse through coercion to perform procedures or performing procedures without consent. … Obstetric racism emerges specifically in reproductive care and places Black women and their infants at risk.”
In analyzing the responses of 214 Black women who participated in the 2018 Listening to Mothers in California Survey, researchers found that one in ten Black women felt they were treated unfairly during their hospital stay due to racism, and one in ten felt they were roughly handled or experienced rude or threatening language from a provider (NPWF 2018).
One third of Black women who participated in the survey felt that delivery room staff did not encourage them to make choices about their birth progression (compared to one out of five of white respondents), and more Black women than white women reported feeling pressured into having medical interventions during childbirth from medical providers (NPWF 2018).
You can learn more about racism and anti-racism in birth care and birth work by visiting our Signature Article, Evidence on: Antiracism in Health Care and Birth Work.
For these reasons, access to continuous labor support from a doula or other labor support professional is especially vital for Black, Indigenous, and birthing families of color. A 2022 analysis of responses from 1,977 women in the 2018 Listening to Mothers in California survey found that women of color and those who received Medi-Cal insurance who reported having a doula present with them during birth were more likely to report experiencing respectful care during labor and birth than those who did not (Mallick, Thoma, & Shenassa 2022).
The results from Mallick et al. are unique because this is one of the first studies to measure the relationship between having a doula present at birth and the likelihood of childbearing people from financially or socially marginalized groups experiencing respectful care. The odds of non-Hispanic Black women with a doula reporting respectful care were 2.7 times higher than those of non-Hispanic Black women without a doula. And the odds were 2.3 times higher for non-Hispanic Asian and Pacific Islander women who had a doula compared to those who did not (Mallick, Thoma, & Shenassa 2022).
Culturally Congruent Doula Care
Who your doula is can also matter a great deal. Some may wish to work with doulas who share their racial, ethnic, or cultural identity. A common theme in qualitative research with doulas of color is the complaint that large doula training organizations do not emphasize race, racism, or how to meaningfully protect people who might experience racism in their birthing experience, in their training curricula. The lack of cultural competency in trainings is a problem for not only doulas but the clients they hope to serve (Thomas et al. 2023). Doulas of color have also developed their own doula education programs specifically to transform the profession and to offer their wisdom as a resource to prospective doula trainees.
Doulas serving families of color need to understand the possibility of harm in the birth room, how to offer real protection and support, and how to acknowledge the fear many families face in simply choosing to have child. If emotional support is a key feature in doula care, doulas cannot fully do their job when they don’t understand or know how to address these fears and anxieties in birthing families. Doulas of color spoke to researchers about how race can influence their connections with clients, and how Black clients who experience obstetric racism often lose trust in medical staff and prefer that doulas who share their identity be their advocates (Sayyad et al. 2023; Thomas et al. 2023).
In one study of community-based doulas who primarily served Black birthing women, the doulas shared how some of their clients did not feel comfortable working with white doulas and prefer to work with doulas who shared their background. This feedback informed how organizations match doulas with clients (Wint et al. 2019). In that same study, researchers found that sharing an identity was not always enough—sharing similarity in life experience or cultural background is also important (Wint et al. 2019).
Having a doula who speaks your language is also important for families who are members of linguistic minorities within a community. In one study of perinatal care for resettled refugees (ethnic-identified Karen women from Myanmar and Thailand), researchers found that Karen-speaking doulas helped Karen-speaking women communicate with doctors (LaMancuso, Goldman, & Nothnagle 2016). Community doulas and community-based doula programs are especially important for migrant and refugee women who are navigating labor and birth in a new country and in their non-native language (Khaw et al. 2022).
Ireland et al. (2019) reviewed research among Indigenous doulas from 19 articles that included a total of 191 Indigenous research participants. They found that Indigenous doulas can help protect Indigenous women from harmful elements of state obstetric policies that may require Indigenous women to birth far away from their support networks.
Indigenous doulas can support their Indigenous clients by bringing longstanding cultural knowledge regarding childbirth into biomedical spaces (Ireland et al. 2019). In a 2021 study with Indigenous doulas working in Canada, researchers found that Indigenous doulas viewed their own presence in the birthing room as a form of ‘harm reduction’ in the present. The doulas hoped their harm reduction would be no longer needed in the future, once more Indigenous midwives and medical professionals are available to Indigenous families. The Indigenous doulas also emphasized the need for one’s Indigenous culture, language, and traditions to be present in the birthing space to protect the well-being of Indigenous birthing families (Cidro et al. 2021).
Benefits of Doula Care for Birthing Families of Color
In another study, researchers conducted in-depth interviews with racially/ethnically diverse, low-income pregnant women to understand how doula support can help women of color (Kozhimannil et al. 2016).
The researchers analyzed the women’s responses around five main themes:
- First, they found that doulas play an important role in agency. Agency is defined as the capacity of individuals to act or to make their own choices. Doulas helped their clients to understand their options and they facilitated communications with care providers, so that clients felt a sense of empowerment or ownership over their care.
- Doulas also contributed to feelings of personal security. When women felt scared by their care providers, they were comforted and reassured by their doulas.
- There was a consensus in the interviews that a doula’s presence facilitated greater respect and autonomy in decision-making.
- Doulas also played a critical role in transferring knowledge about the pregnancy and birth process. They connected clients with resources and “translated” information received from care providers during clinic visits.
- Finally, doulas helped women with connectedness so that they would not feel socially isolated. Many of the participants described stressful life situations and desired a doula with similar life experiences, someone who shared their culture and background.
Sadly, those who can benefit the most from doula care often have the least access. In the 2020s, some state and private health insurance plans began offering reimbursement for doula care. Black, Indigenous, and doulas of color were not always consulted or centered in doula-focused legislation or policymaking. This led to inequitable reimbursement rates that typically do not pay a living wage. Here at EBB, we want to amplify the 7 Demands for Black Doula Day™. Equitable, sustainable wages and reimbursement practices for doulas benefit everyone by keeping doulas working and providing care.
How can doulas support LGBTQI+ Birthing People and Families?
“Pregnancy and childbirth were very male experiences for me. When I birthed my children, I was born into fatherhood.” (Light et al. 2014)
Lesbian, gay, bisexual, transgender, queer, and intersex (LGBTQI+) birthing people and families have pathways to pregnancy and experiences with birth and postpartum care that may be beyond the training and skills of some medical providers, and doulas can support them in accessing accurate, high-quality, and respectful care. All health care providers and birth workers, including doulas, should educate themselves about how to best meet the needs of LGBTQI+, queer, and gender diverse families during pregnancy and childbirth (MacTavish 2011).
From the 1970s through the 2010s, doula work was historically focused on white, cisgender, heterosexual women’s experiences in childbirth (Morgen 2002; Morton & Clift 2014). For many years, the most used birth resources, the most popular birth books, and much of the language used by doula training organizations promoted the idea that birth is solely the domain of cisgender, straight women.
But it is important to avoid using exclusively stereotypical language about pregnancy and birth that assumes all people are cis-gendered and heterosexual. Instead, LGBTQI+ advocates urge us to include all the identities, families, and pathways to pregnancy that LGBTQI+ people take (Yam & Fixmer-Oraiz 2023). Some doula training organizations, such as Birthing Advocacy Doula Trainings (BADT), help promote a truly inclusive approach to doula support in childbirth and host trainings that address the needs of diverse families, including queer and trans birthing people.
Unconditional support from doulas is even more important given that many health care providers discriminate against LGBTQI+ people. This can look like a refusal to use a person’s chosen name or their pronouns, being dismissive towards their family structure, being condescending about their partner’s identity, or relying on stereotypes rather than a person’s individual needs and experiences in providing care. Furthermore, our health care systems do not provide easy access to proper medical care for LGBTQI+ families during pregnancy, pregnancy loss, and childbirth (Karrington 2021; Light et al. 2014; Thornton & Mattatall 2021; Wojnar 2007).
Many trans men who choose to give birth will seek midwifery care or doula care because these models of care can support them in maintaining bodily autonomy and a sense of control during childbirth (Besse, Lampe, & Mann 2020). In a small study of the pregnancy experience of 41 transgender men, researchers found that 22% of the participants gave birth outside of a hospital, and 46% sought prenatal care from midwives (Light et al. 2014). Non-binary individuals assigned female at birth may face additional hurdles to seeking informed, respectful pregnancy care due to the lack of research, resources, and education on their specific needs and how these may differ from those of trans men (Fischer 2021).
Doulas can support LGBTQI+ families in several ways, including (Heggie et al. 2023; MacTavish 2011; Yam & Fixmer-Oraiz 2023):
- Using inclusive language when talking about pregnancy, birth, and postpartum in general, and using a client’s preferred terminology when supporting them.
- Advocating for LGBTQI+ birthing people and their families in medical settings. This can look like reminding hospital staff to use the correct pronouns and inclusive terms when speaking to a birthing person or their partner.
- Communicating with medical providers (per the birthing person’s wishes) and offering additional explanation if needed in case of questions about relevant medical history that could impact their medical decision-making.
- Self-education and adequate preparation to provide support to LGBTQI+ birthing people is essential. Doulas should seek out trainings and continued education about LGBTQI+ pregnancy and birth care to keep up with the best practices to support this community.
- Connecting LGBTQI+ families to LGBTQI+ birth workers active in their community is another important way to ensure that families receive culturally congruent supportive care during pregnancy and birth.
- Advocacy for LGBTQI+ birthing people and families can extend beyond the hospital. Doulas can work with other doulas and within the broader birth work community to remove gender stereotyping language from trainings, and to reject transphobia, homophobia, queerphobia, and cissexism in doula and birth workspaces.
These are just some examples of the types of knowledge and skills that doulas need to have to effectively serve this diverse community. The research on LGBTQI+ doula care is limited, but it appears that many LGBTQI+ families may seek out doula support or midwifery care because of fears of facing homophobia, transphobia, or mistreatment from the medical community, or because of a greater need for advocacy during pregnancy and birth.
At the end of this article, we include resources that LGBTQI+ birthing people and families, and LGBTQI+ doulas can use to connect with one another.
Are doulas welcome at every hospital?
Even though doulas improve birth outcomes, many hospitals around the world do not welcome their presence. Researchers have been studying what the barriers to doula care are, in hopes that we can overcome these obstacles.
In 2019, a Cochrane review (Bohren et al. 2019b) asked how birthing people, partners/family, and health care workers felt about working with doulas. They also asked, why is continuous support not provided more often, given the many research benefits that have already been published? The three main goals of this study were to:
- Describe how the entire birth team feels about the presence of a labor companion.
- Identify why some places are better able to include labor companions.
- Support and build on the findings from the 2017 Cochrane review on labor companions.
The 2019 review combined 51 qualitative studies (text data from interviews and focus groups) published in English, French, Spanish, Turkish, and Norwegian. The studies were located across 23 countries, including 17 studies in North America, 14 in Europe, 7 in Africa, 5 in the Middle East, 3 in South America, 3 in Oceania, and 2 in Asia, and covered high, medium, and low-income settings.
The researchers stated the overall quality of the evidence as high or moderate, according to the GRADE-CERQual system of rating qualitative evidence. Different types of continuous support were included, ranging from lay companions such as a male partner, female relative, or friend, to trained doulas or student midwives. Support could be given only during labor, or in a model that includes prenatal and postpartum visits. Most studies described what it felt like for a birthing person to have a continuous support person with them in labor. Some studies shared perspectives from partners, nurses, midwives, and/or doctor, or other key stakeholders such as hospital administrators and policy makers.
Three key themes helped explain why doulas are not yet standard in birth:
- Labor support and emotional support are still perceived as lower priorities than physical health and medical care, especially in low-resource areas.
Labor support may be viewed as “nice to have,” but not essential, especially in communities with low resources. Some people on the birth team, even the person giving birth, may feel that emotional and physical support strategies like hand holding, massage, or encouragement are unnecessary, or could be done by a nurse or other hospital staff. Especially in smaller buildings, it is thought that there is not enough space, beds, or chairs for labor companions. In places where a labor companion is required to wear hospital attire, resources may be too low to provide the clothing. Although the evidence shows that this kind of support improves birth outcomes both for parents and babies, in low resources settings where there is limited access to even lifesaving procedures, this level of care can be seen as pulling time and resources away from saving lives.
- Not all birth settings welcome labor companions.
Many birth settings still formally forbid labor companions from being part of the birth team. Labor support will not be possible in these settings until a formal policy change is made, shared with families, and health care providers are informed that they must comply with the new policy. Still, competing priorities can arise, such as fear of labor companions increasing the risk of infection, lack of space on days when the labor unit is crowded, or privacy concerns around male companions in areas with open floor plans (where only thin curtains separate patients from each other). For example, in Brazil, labor companions are allowed at all births by law, but some providers refuse to allow a companion to enter the room if they think the companion is unprepared or needs “supervision,” or if the patient is poor or uninsured.
- Health care staff are not prepared to work together with doulas or value what they bring to the team.
Nurses, midwives, and doctors can have prejudices that lead to them resisting the presence of doulas or labor companions. Doulas bring a unique perspective into the birth room that may be perceived as “clashing” with the way hospital staff approach birth. Hospital staff may see themselves as superior because of their years of training, strict protocols, and practice guidelines in physical health and medical care that they are supposed to follow. To them, a lay person coming in to support labor and offer emotional care can seem unprepared, untrained or “anti-medical establishment.” Instead of focusing on rules, policies, and medical emergencies, doulas provide companionship, informational support, emotional support, a sense of safety and calm, and advocacy, which can be seen as at odds with health care staff who have specific tasks that they want to accomplish and a goal of patient compliance with hospital policies and protocols.
In the eyes of hospital staff, doulas can be seen as lacking purpose or appropriate boundaries, or as someone who “gets in the way.” Providers think they must “manage” this extra person, adding to their already full workload, and they may fear being evaluated, misunderstood, or judged for their clinical decisions by someone they view as having no understanding of birth physiology or medicine. Some midwives and nurses may worry that doulas will take over their caring and nurturing role, which may be one of the reasons why they chose this field, while others may appreciate the extra help so that they can better focus on clinical tasks.
Labor companions can also feel frustrated by not having enough training or direction on how to help with difficult births or how to interact with medical staff. They may offer advice or intrude on the roles of medical staff if they think their client’s safety or birth preferences are at risk. They may notice when they are not valued by medical staff, and become defensive to all future medical providers, anticipating challenges and successfully navigating their role, but at the cost of losing hope for creating collaborative partnerships with medical providers.
Doulas and health care staff each address a different and important element of caring for someone in labor. When they are trained on how to respect each other’s roles in a spirit of cooperation rather than conflict, most providers agree that doulas are a valued part of the birth team. But when doulas are not well integrated, they can be ignored and actively excluded from care giving. Providers may feel frustrated, unsure how to “manage” the doula, and fear that their patients with doulas will create conflict, have more physical pain, or refuse to follow medical advice.
Here at EBB, we have witnessed another phenomenon, which is that some providers do not believe someone can give birth without another person in control of them and their choices. These providers assume that the doula is there to “control” the birthing person in place of the doctor. They may see the birthing person’s autonomous choices as being made by the doula simply because a doula is present. This perception leads the provider to view the doula as a threat to the provider’s need to have authority over the birthing person.
Based on the 2019 Cochrane review, here are seven questions to find out how well prepared a birth setting is to welcome birth companions:
- Are providers trained on the benefits of labor companions?
- Are patients educated on the benefits of labor companions?
- Is the birth setting structured in a way to ensure privacy?
- Are providers trained on how to include companions as valued members of the birth team?
- Are there clear roles and expectations for both companions and providers?
- If your companion is a lay person (and not a trained doula), does your birth setting offer prenatal training to help your companion learn how to provide labor support?
- Is the pregnant person permitted to choose their own companion(s)?
If having labor support is important to you, please share the evidence from this Signature Article on Doulas with your providers, so that doulas can be more integrated, understood, and welcomed in the future.
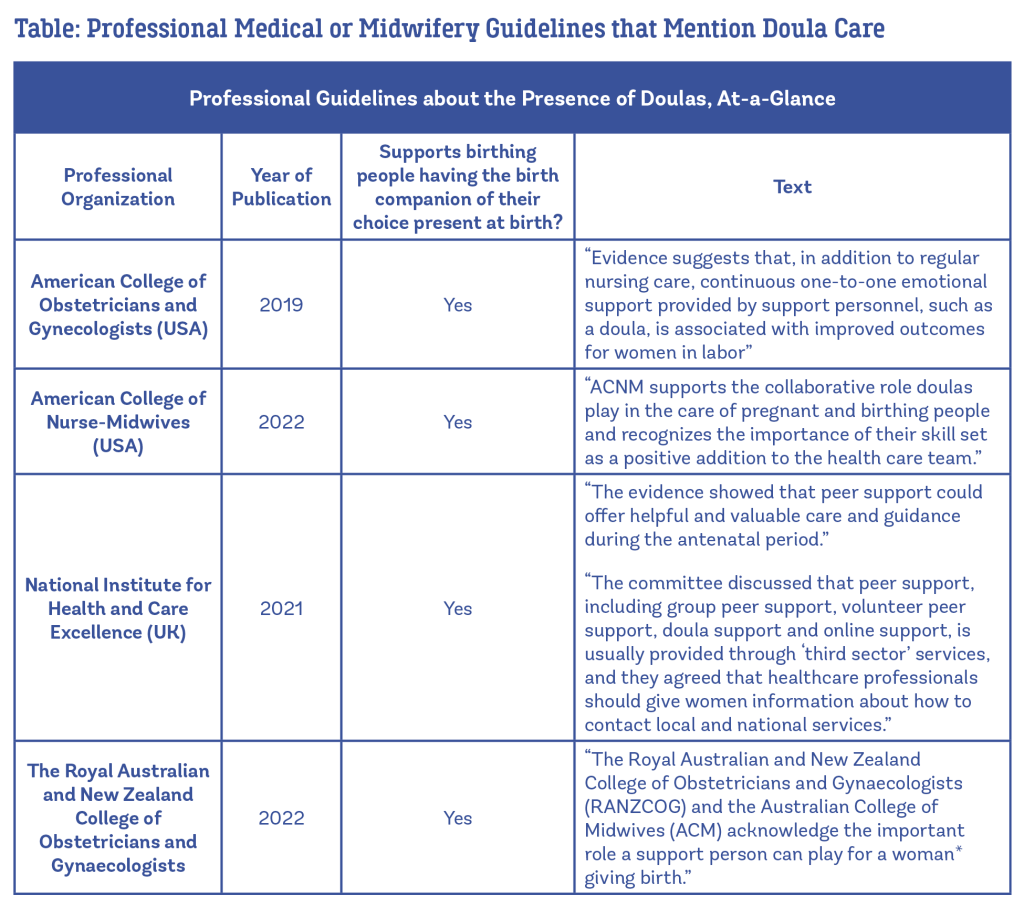
Other global issues faced by doulas
Doulas practice in hospitals and birthing centers and at home births around the world. While a passion for birth and for supporting birthing people may unite doulas, the everyday experience of being a doula can vary significantly.
In many countries, medical professionals are still not familiar with doulas or what they do. This means many medical professionals are uncomfortable with the presence of a doula in the labor room. In some medical systems, the presence of a birth companion is not always allowed, and birth companions can be easily dismissed from the labor room, which can make it difficult for doulas to provide continuous support and care during labor and birth.
Many doula trainings are based in North America or Europe or developed by organizations based in these regions. As a result, the trainings and resources provided by these organizations may not be applicable to the experiences and needs of doulas and clients who come from different cultures, or who are working and birthing in different medical systems.
In the resources section at the end of this article, we include resources about how to find a doula, as well as links to EBB podcasts with doulas around the world.
What is the bottom line?
Evidence shows that continuous labor support is one of the most important and basic needs of birthing people. And evidence clearly shows that a doula’s presence improves birth outcomes! Continuous labor support can lower the chances of needing a Cesarean, lower the use of medications for pain relief, and lower the risk of newborns experiencing a low five-minute Apgar score (Bohren et al. 2017; Gilliland 2010b; McGrath & Kennell 2008; Nguyen & Heelan Fancher 2022).
Doulas improve birthing people’s satisfaction with their birth and provide an important source of physical, emotional, informational, and advocacy support for both the birthing person and their birth partner(s) (Bohren et al. 2019b; Johansson 2015; Mallick, Thoma, & Shenassa 2022). Doulas are not medical professionals, but their value in making childbirth safer and more supported has been recognized by leading professional medical organizations and by nurses and other medical staff who report having positive attitudes towards doulas (Ballen & Fulcher 2006; Neel et al. 2019).
Research has not shown any medical risks to having a doula. However, there may be some potential drawbacks if the birthing person has expectations of advocacy that their doula is unable to fulfill. In addition, when working with any professional, there is the risk that the person you hire may not fulfill their obligations to you. Speaking to a doula’s former clients is an important way to vet your doula.
Doulas are a diverse group with a range of perspectives on and approaches to birth. Not every doula is the best fit for every birthing family—you may need to meet with several before you find the right person. Likewise, doulas may decline to work with a client who has expectations they cannot fulfill, who behaves towards them in an abusive or inappropriate manner, or who is otherwise dishonest towards them in their dealings. Before signing any agreement, it is important for the doula and the client to both clearly outline their expectations and approaches to birth and come to a mutual understanding.
Doulas are trained to provide support to birthing people during pregnancy, labor, and birth—but they do so much more! Doulas engage in a wide range of forms of care and support. Some doulas care for people prior to conception, during abortions, during and after a miscarriage, in the weeks after childbirth, and at the end stages of life. There are many different types of doulas, who draw on many different types of trainings, certifications, traditional cultural or faith-based practices, and perspectives on childbirth in their work to support birthing people before, during, and after childbirth.
Research shows what many families already know: a doula can make a big difference in your childbirth experience. However, having a doula is not a magic wand. Doulas often work in broken health care systems in the face of oppression, racism, homophobia, transphobia, and other “isms.” Doulas need all our support in advocating for safer, more supportive birth settings. The doula’s role can also be made more difficult if you and/or your birth partner(s) have limited knowledge about birth options when you go into labor. Educating yourself about birth as much as possible beforehand can equip you with skills that will enhance the doula’s labor support.
For those considering becoming a doula, it is important to consider what types of training you want to pursue and what your own approach to this type of birth work will be. It is also important to recognize that this can be a demanding field where you may be exposed to challenging situations and traumatic births. Seeking out community support from other doulas can help you to process difficult emotions and avoid burnout.
In conclusion, doulas provide important benefits for their clients, birthing families, and communities, as well as for hospitals and medical systems. Therefore, doulas should be viewed and valued by both parents and providers as valuable, evidence-based members of the birth care team, whose presence can improve health outcomes for parents and babies.

How do I find a doula? + Interview questions
Finding a doula can feel daunting, but there are a lot of great resources available that help connect pregnant people to doulas working in their region. In the “Other Resources” section below, we provide a list of websites with directories of doulas working in the U.S., Canada, the UK, Australia, India, as well as some directories with international listings. There are many directories and websites to choose from in addition to the ones listed in the resources section. You may be able to find a directory of doulas working in your state or city by searing [State/City] + doula.
Another great way to find a doula is through word of mouth. If you know someone who has recently given birth and worked with a doula you may want to ask them about their experience. Your midwife or OBGYN practice may be able to recommend doulas who have worked in your birth center or hospital previously. Your childbirth educator may be another great person to ask.
In the U.S., some states may offer Medicaid reimbursement for doula services or may have other programs available to connect their residents with doulas. Likewise, some insurance plans offer reimbursement for doula services, or may allow you to use your Health Savings Account (HSA) to pay for a doula. Before hiring a doula, you may want to learn more about what state programs or insurance options are available to you.
If you’re at all on the fence about hiring a doula, you may want to interview several doulas with your birth partners(s). We have created a set of questions that you can use to prepare to meet with a doula and to help you and your partner decide what doula might be the best fit for you.
- Questions to ask yourself
- What does support look like for me?
- What kind of support team do I want at my birth?
- What types of support do I feel like I need?
- Advocacy support? Emotional support? Physical Support? Informational support?
- When do I need support?
- Prior to conception? In early pregnancy? In labor only? After I give birth?
- Is hiring a doula an option?
- What resources can we use? Are there community-based doula programs in my area? Does my hospital have a free doula program?
- Is doula care covered by my health insurance?
- Is doula care covered by my state health insurance?
- Questions to discuss with your birthing partner or family
- Do they know what a doula is?
- What questions do they have about doulas?
- Does my birthing companion need support from the doula during birth? What type of support might they need from a doula?
- Doula interview questions
- Background:
- What type of training(s) have you completed?
- Which doula organizations are you affiliated or certified with?
- How long have you been practicing as a doula?
- How many births have you attended?
- Have you attended any births at the birth center/hospital where I plan to have my baby? OR: Have you worked with my homebirth midwife before?
- Do you provide any other type of birth work (lactation consultant, childbirth education, etc.)?
- Do you have former clients that can provide a reference?
- Philosophy
- Can you tell me about the type of support that you offer to your clients?
- Can you tell me about the role advocacy plays for you in your work as a doula?
- What does being a doula mean to you?
- What do you do if your perspective on birth differs from that of your client?
- Practical Questions:
- Can you tell me about the services that you provide?
- Do you provide childbirth education? Do you recommend a childbirth education class?
- How many times will we meet before birth/after birth?
- How will we communicate in the time leading up to my birth?
- When would you plan to come to me when I am in labor? How long will you stay?
- What is the backup plan if you are unable to attend my birth? If my labor is unusually long?
- Do you have any supplies that you will bring that you might use while I am in labor? (TENS machine, aromatherapy, etc.)
- Do you work with other doulas?
- Can you describe how you interact with medical providers during a birth?
- Can you tell me about your fees?
- What services does your fee cover?
- Are there additional services that you provide for an additional cost?
- Do you take health insurance? Do you take a payment plan?
- After the meeting
- Check in with yourself—how did the meeting make you feel? How does your partner/birth companion feel?
- Do you feel comfortable with this doula?
- Does this doula’s approach align with your needs?
- Do you have any questions or concerns?
- Can you tell me about the services that you provide?
- Background:
EBB Resources for Doulas & Families
For more information about community-based doulas, visit these EBB Podcast Episodes:
- EBB 92 – Impacts of the Community Birth Worker Model with Aza Nedhari
- EBB 191 – Cultural Awareness in Birth and Postpartum Work with Community Doula Marnellie Bishop
- EBB 229 – Evidence on Doulas: Community-Based Models, the Pandemic and Reimbursement with the Research Team
- EBB 260 – Midwifery, Community Birth Work, and Plant Medicine in Louisiana with Ms. Divine Bailey-Nicholas, the Founder of Divine Birth Wisdom
For more information about postpartum doulas, you can check out these EBB Podcast Episodes:
- EBB 191 – Cultural Awareness in Birth and Postpartum Work with Community Doula Marnellie Bishop
- EBB 271 – Bringing a Whole Family Approach to Birth and Postpartum Doula Work with Brandi Jordan, Founder of The Cradle Company
- EBB 288 – From Birthing in the Pandemic to Birthing a Career as a Postpartum Doula and Chef with Malisa Dekker of Planted Postpartum
For more information about full spectrum doulas, you can check out these EBB Podcast Episodes:
- EBB 195 – Grief and Healing Through Pregnancy and Infant Loss with Full Spectrum Doula, Rose Rankin
- EBB 207 – Gender-Affirming Birth Work and Education with Full Spectrum Doula and Childbirth Educator, Moss Froom
- EBB 263 – Birthing Liberation with author, CEO, educator, full spectrum doula, and Black Luxury expert, Sabia Wade
- EBB 272 – Navigating Assisted Reproduction & Full Spectrum Childbirth Support with EBB Childbirth Class Graduate, Jessica King
For more information about doulas of color and anti-racism in birth work, you can check out these EBB Podcast Episodes and more:
- Signature Article, The Evidence on: Anti-Racism in Health Care and Birth Work
- EBB 191 – Cultural Awareness in Birth and Postpartum Work with Community Doula Marnellie Bishop
- EBB 228 – Uplifting Radicalized Birth Work with Anna, The Pocket Doula
- EBB 252 – A Candid Conversation about Doula Advocacy with Doula and EBB Instructor Leslie Greene
- EBB 263 – Birthing Liberation with author, CEO, educator, full spectrum doula, and Black Luxury expert, Sabia Wade
- EBB 270 – Intersectionality and Representation in Birth Work with Cheyenne Varner, Doula and Founder of The Educated Birth
- EBB Podcast 293 – Decolonial Approaches to Birth and Supporting Survivors with Eri Guajardo Johnson of Birth Bruja
For more information about global doula practice, you can check out these EBB Podcast Episodes:
- EBB 126 – Finding the Right Provider and Birth in the Dominican Republic with Leiko Hidaka.
- EBB 259 – Cross-Cultural Experiences in Childbirth with Ruth Greene, Doula and Co-owner of Having a Baby in China Consulting Services
- EBB 306 – Culturally Sensitive Doula Training with Divya Deswal and Neha Misra of the Doula Collective in India
For more information about LGBTQI+ Doulas and supporting LGBTQI+ Birthing families, you can check out these EBB Podcast Episodes:
- EBB 207 – Gender-Affirming Birth Work and Education with Full Spectrum Doula and Childbirth Educator, Moss Froom
- EBB 227 – Amplifying the Need for Intersectional Birth Support for QTBIPOC Birthing People with Xian Brooks of the Dandy Doula
- EBB 228 – Uplifting Radicalized Birth Work with Anna, The Pocket Doula
For more information about doulas and the business of doula work, you can check out these EBB Podcast Episodes:
- EBB 229 – Evidence on Doulas: Community-Based Models, the Pandemic and Reimbursement with the Research Team
- EBB 271 – Bringing a Whole Family Approach to Birth and Postpartum Doula Work with Brandi Jordan, Founder of The Cradle Company
- EBB 285 – Creating a Sustainable Career in Birth Work with Jessica Diggs, Midwife, Doula Mentor, and Co-Founder of Centered
- EBB 288 – From Birthing in the Pandemic to Birthing a Career as a Postpartum Doula and Chef with Malisa Dekker of Planted Postpartum
Other Resources (including Doula Directories)
Doula of Color directories:
- SistaMidwifeDirectory.com
- Black Doula Locator from Black Women Birthing Justice
- Irth App: Resources
- Doula Match: Indigenous/Aboriginal doula directory
- Doula Match: Black doula directory
- National Black Doulas Association directory
General Websites and directories for finding a doula:
- Birthworks International
- CAPPA International Directory
- Doula Match
- DONA International: Find a Doula
- The Doula Collective (India): Directory
- Doula Trainings International: Directory
- Hello Meela: Find a Doula
- Doula.org UK: Find a Doula
- Doula Training Canada: Directory
- Fat and Pregnant Size Inclusive Birth Professional Directory
- Find a Doula (Australia)
Doula of color resources:
- The National Black Doulas Association
- Birthworkers of Color Collective
- ekw’í7tl doula collective
- Birth Companions Community Center
- Ancient Song Doula services
- National Association to Advance Black Birth
- National Black Doula Day™ (https://blackdouladay.com)
End-of-life doula resources:
Other Full spectrum doula resources:
- The National Partnership for Women & Families: “Our Communities Hold the Solutions” The Importance of Full-Spectrum Doulas to Reproductive Health and Justice
- NPR Fresh Air: “Full-Spectrum” Doula On Birth & Abortion
Additional LGBTQI+ Doula resources
References:
Acknowledgment
We would like to extend our gratitude to our expert reviewers for valuable feedback and critique of this article before publication: Rhonda Fellows CAB-CD, Doula Trainer- Community Aware Birthworker, Pelvic Steam Facilitator, Evidence Based Birth®️ Instructor; Heather Christine Struwe PT, Birth Doula Trainer- Community Aware Birthworker, Evidence Based Birth®️ Instructor, and Cristen Pascucci, founder of Birth Monopoly. The photos featured in this article are from: Birth Becomes Her, @see_baby, @bellaariella, and @omorosebless.
Birth Professionals:
Join others who also want to help bring evidence-based care to their local community.
Also, gain complimentary access to a printable library of our Signature Articles, 20+ hours of CE courses, a private community, and more.
Buy EBB Inspirational T-shirts, Due Date Buttons & Birth Affirmation Cards




Stay empowered, read more :

EBB 308 – The Intersection of Environmental Justice and Midwifery Care with Dr. Tanya Khemet Taiwo
Don't miss an episode! Subscribe to our podcast and leave a review! iTunes | Spotify | YouTube Curious which toxins should be most avoided for people of reproductive age and their children? In this episode, Dr. Tanya Khemet Taiwo, LM, CPM, MPH, PhD unravels the...
EBB 307 – Unexplained Infertility, Endometriosis, and a Birth Center Birth Story with Ellora La Shier, EBB Childbirth Class Graduate
Don't miss an episode! Subscribe to our podcast and leave a review! iTunes | Spotify | GoogleIn this episode, Ellora La Shier, graduate of the EBB Childbirth Class, shares about her struggle with six years of unexplained infertility and how it impacted her...

EBB 306 – Culturally Sensitive Doula Training with Divya Deswal and Neha Misra of the Doula Collective in India
Don't miss an episode! Subscribe to our podcast and leave a review! iTunes | Spotify | Google As we wrap up the celebration of World Doula Week, explore the transformative journey of pregnancy and childbirth in the Indian context with Divya Deswal and Neha Misra,...